


For many years, members of the medical establishment have considered abstinence the only acceptable goal of Alcohol Use Disorder (AUD) treatment, even though some controlled drinking might be an appropriate goal for some AUD patients. As a result, many patients with AUD have been unable to set their own treatment goals. There is growing evidence that individuals with AUD want to have an active or shared role in decision-making for their treatment, instead of leaving treatment decisions to the sole judgment of their doctors. This week, The DRAM reviews a study by Anke Friedrichs and her colleagues that explored the treatment decision-making preferences of patients with AUD.
What was the research question?
Are AUD patients’ decision-making preferences linked to their motivations for seeking treatment?
What did the researchers do?
The researchers collected data from 242 people who were seeking treatment for Alcohol Use Disorder. Before beginning treatment, each participant indicated their preference for either making their own treatment decisions (informed decision-making), making treatment decisions with their doctors (shared decision-making), or allowing their doctor to make treatment decisions for them (passive decision-making).1 The participants also completed a questionnaire about the severity of their addiction and their motivation for treatment, which included their desire for help and their treatment readiness (i.e., the extent to which a person has committed themselves to actively pursuing treatment). The researchers analyzed this data using logistic regression to see whether any variables were associated with preferring one type of decision-making over another.
What did they find?
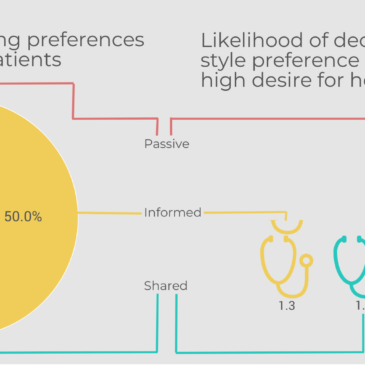
The vast majority of AUD patients preferred to have either sole (50.0%) or shared (39.7%) responsibility for making their own treatment decisions. Participants who scored high on the “desire for help” scale were significantly more likely to prefer passive decision making, compared to shared decision-making. No other variables were associated with decision-making preference.

Figure. The pie chart indicates the proportion of AUD participants preferring each type of decision-making.The stethoscopes indicate the likelihood of a participant preferring informed or passive decision-making (in comparison to shared decision-making) depending on their desire for help. Click image to enlarge.
Why do these findings matter?
To the extent that these participants represent all AUD patients, this study indicates that most AUD patients prefer to be involved in decisions about their treatment. There is some evidence that people with AUD believe that they are better able to meet their treatment goals when those goals are self-selected. Healthcare providers should ask their AUD patients how they prefer to make their treatment decisions as this might help establish a better rapport and allow patients to be more invested in their treatment.
Every study has limitations. What are the limitations in this study?
All of the participants in this study sought AUD treatment at one of four German psychiatric clinics. This means that the treatment preferences of these AUD patients might not be representative of AUD patients outside of these clinics or in other countries.
For more information:
If you are concerned about your alcohol use, Your First Step to Change is a free online resource that can help you figure out whether and how to change.
— Rhiannon Chou Wiley
What do you think? Please use the comment link below to provide feedback on this article.
________________
1 Participants indicated their decision-making preference by agreeing with one of the following statements:
-
- Passive role preference: “I prefer to leave all decisions to my doctor” or “I prefer that my doctor make the final decision after considering my opinion”
- Shared role preference: “I prefer that my doctor and I share responsibility for deciding which treatment is best for me”
- Informed decision-making role preference: “I prefer to make the final decision” or “I prefer to make the final decision after considering my doctor’s opinion.”
Mike Ashton January 9, 2019
We looked at the relation between these kinds of preferences, therapist directiveness and addiction treatment outcomes in “My Way or yours?”, freely available at:
https://findings.org.uk/PHP/dl.php?file=Ashton_M_35.pdf&s=ml
It was part of the Manners Matter series – see all at:
https://findings.org.uk/issuesResults.php?s=ml&issueChoice=series+3
The conclusion was that matching client preferences to therapist style can be an important factor in treatment success.