


Studies linking childhood sexual abuse (CSA) to higher likelihood of alcohol dependence (AD) later in life (i.e., Dinwiddie et al., 2000; Fergusson, Horwood, & Lynskey, 1996; Kendler et al., 2000; Kilpatrick et al., 2000; Molnair, Buka, & Kessler, 2001; Nelson et al., 2002) might lack adequate control for environmental and genetic factors that influence the relationship between CSA and AD. These studies are also inconclusive because an earlier age of first drink is associated with later AD regardless of CSA status (DeWit, 2000). This week’s DRAM reviews a study that controls for the influence of environmental and genetic characteristics, as well as the influence of drinking at an early age using a sample of twins.
Sartor, Lynskey, Bucholz, McCutcheon, Nelson, Waldron, et al. (2007) conducted telephone surveys with 2061 (response rate 78%) 18-29 year old female monozygotic or dizygotic twin sets participating in the Missouri Adolescent Female Twin Study (Heath et al., 2002). The survey included the Semi-Structured Assessment for the Genetics of Alcoholism (SSAGA; Bucholz, 1994; Hesselbrock, 1999), age at first drink, age of onset of AD, and Traumatic Events and Early Childhood Experiences. Participants met researchers’ criteria for CSA if they endorsed having experienced rape, sexual molestation, and/or forced sexual contact before age 16, or sexual contact by someone five or more years older before they reached age 16. The authors measured speed of progression to AD by measuring age at first drink and age at onset of AD.

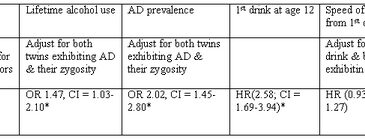
Figure. Alcohol use measures adjusted for environmental, genetic, or early age of first drink correlates among those with CSA history (adapted from Sartor et al., 2007). Click image to enlarge.
* Significant
** OR = Odds ratio, HR = Hazard ratio
The sample was 86% Caucasian and 14% African American. Almost 12% endorsed a history of CSA and 7.9% qualified for AD. The authors adjusted for the genetic influence expressed by the higher risk for AD if her twin had AD, especially if they were monozygotic twins. After adjusting for genetic factors, CSA was associated with a greater likelihood of lifetime alcohol use, having a first drink at an early age, and AD (see Figure). However, the effect of CSA on AD was mediated by age at first drink. After adjusting for the genetic influence on AD and the CSA-related age at first drink, CSA history did not increase the speed of AD onset from 1st drink.
The study was based on self-report and defines CSA narrowly; these factors might lead to under reporting CSA. Rather than compare sets of twins where only one female experienced CSA, researchers group all twins together, and then statistically controlled for differences between twin pairs. This yields a larger sample size and, therefore, statistical significance for smaller differences. The study did not report the rate of co-occurrence in twin pairs of CSA and AD, and congruence across twins. Adjusting for AD co-occurrence might adjust for CSA co-occurrence if congruence is common. The results might not generalize well to the general population because a very small subset of the overall sample had both a history of CSA and AD; the entire sample was female, and most of the sample was Caucasian.
Contrary to expectation, CSA did not predict time to AD after adjusting for age at first drink. Drinking at an early age predicted a more rapid pace for AD development; however, both twins having AD was the best predictor of rapid onset of AD after their first drink, suggesting genetics and environment are greater risk factors for this effect than CSA. Future research could examine an early intervention’s effectiveness for reducing rates of later AD among early adolescents reporting CSA history.
—Leslie Bosworth
What do you think? Please use the comment link below to provide feedback on this article.
References
DeWit, D., Adlaf, E.M., Offord, D.R., Ogborne, A.C. (2000). Age at first use: a risk factor for the development of alcohol use disorders. American Journal of Psychiatry, 157, 745-750.
Dinwiddie, S., Heath, A. C., Dunne, M. P., Bucholz, K. K., Madden, P. A. F., Slutske, W. S., et al. (2000). Early sexual abuse and lifetime psychopathology: a co-twin control study. Psychological Medicine, 30, 41-52.
Fergusson, D. M., Horwood, L. J., & Lynskey, M. T. (1996). Childhood sexual abuse and psychiatric disorders in early adulthood. II. Psychiatric outcomes of childhood abuse. Journal of the American Academy of Childhood and Adolescent Psychiatry, 35, 1365-1374.
Heath, A. C., Howells, W., Bucholz, K. K., Glowinski, A. L., Nelson, E. C., & Madden, P. A. (2002). Ascertainment of a mid-western U.S. female aldolescent twin cohort for alcohol studies: assessment of sample representativeness using brither record data. Twin Research, 5, 107-112.
Kendler, K. S., Bulik, C. M., Silberg, J., Hettema, J. M., Myers, J., & Prescott, C. A. (2000). Childhood sexual abuse and adult psychiatric and substance use disorders in women. An epidemiological and co-twin control analysis. Archives of General Psychiatry, 57, 953-959.
Kilpatrick, D. G., Acierno, R., Saunders, B., Resnick, H. S., Best, C. L., & Schnurr, P. P. (2000). Risk factors for adolescent substance abuse and dependence: data from a national sample. Journal of Consulting and Clinical Psychology, 68, 19-30.
Molnair, B. E., Buka, S. L., & Kessler, R. C. (2001). Childhood sexual abuse and the subsequent psychopathology: results from the National Comorbidity Study. American Journal of Public Health, 91, 753-760.
Nelson, E. C., Heath, A. C., Madden, P. A. F., Cooper, M. L., Dinwiddie, S. H., Bucholz, K. K., et al. (2002). Association between self-reported childhood sexual abuse and adverse psychosocial outcomes. Results from a twin study. Archives of General Psychiatry, 59, 139-145.
Sartor, C. E., Lynskey, M. T., Bucholz, K. K., McCutcheon, V. V., Nelson, E. C., Waldron, M., et al. (2007). Childhood sexual abuse and the course of alcohol dependence development: Findings from a female twin sample. Drug and Alcohol Dependence, 89, 139-144.
Randall December 27, 2007
This is an important piece of work, but seems to be missing is a differentiation between “mild” CSA and “traumagenic” CSA. many women have a childhood history of SA, but some were:
-Very young when the abuse began
-Abused repeatedly over a period of years
-Abused by someone they should have been able to trust
-Abused in a more intrusive manner
-Either themselves threatened, or a family member or cherished object threatened with violence
-Blamed or not believed when the abuse was disclosed.
These factors tend to separate a “household” group of CSA survivors (minimal on-going trauma) or “clinical” group (PTSD, generalized anxiety, depression, dissociative disorder, substance abuse or dependency).