


Increases in the availability of legalized gambling have been accompanied by increased concern about youth gambling. Initial empirical reports on the prevalence of youth gambling indicate that this concern might be warranted. A meta-analysis of published studies of college students estimated the prevalence rate of lifetime problem gambling at 5.6% – approximately three times the rate found in the adult population (1.9%)(Shaffer & Hall, 2001). This week The WAGER reports on a recent publication of findings from a longitudinal study of college students in Missouri (Slutske, Jackson, & Sher, 2003).
When the study began, the 468 participants were first-time college first year students: half had a paternal history of alcoholism and half had no history of alcohol or drug abuse among first or second degree relatives because a separate study which drew from this sample required these qualities.1 The sample was 94% White and 54% female. The researchers surveyed the participants, either in person or by telephone, in 1987- 1988 (Year 1), 1990-1991 (Year 4), 1993-1994 (Year 7), and 1998-1999 (Year 11). Participant retention was high: 97%, 94% and 84% for Years 4, 7, and 11, respectively. In Year 1, the researchers determined problem gambling by administering a truncated version of the gambling section of the Diagnostic Interview Schedule (DIS) based on DSM-III. To determine problem gambling in other years, the researchers administered the full gambling section of the DIS based on DSM-III-R at Years 4 and 7 and the full DIS based on DSM-IV at Year 11.
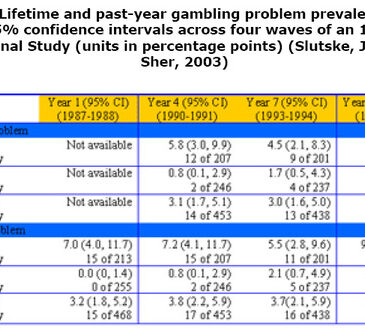
Because the modal number of endorsed problem gambling symptoms was only one for all four years, the researchers were unable to use DSM diagnosic definitions of problem gambling. Throughout the course of this study, only 4 individuals (3 men, 1 woman) met the DSM criteria for pathological gambling. Consequently, Slutske et al. (2003) defined problem gambling in this study as the endorsement of one or more problem gambling symptoms. Table 1 presents the reported participants’ lifetime and past year gambling problem prevalence rates for each wave of interviews.

Results showed that, even when a generous operational definition of problem gambling was used, the full sample lifetime prevalence rates observed at each wave of the college years (Years 1 and 4) were low (3.2%-3.8%) compared with previous findings using standard DSM criteria (5.6%) (Shaffer & Hall, 2001). In the three years it was measured, the pastyear rate of gambling problems was lowest at Year 11 (1.8%), while the period from Year 7 to 11 showed the greatest increase in lifetime prevalence, from 3.7% to 5.3%. This seeming inconsistency could result from either an unusually large increase in new gambling problems, or incongruities in self reports of lifetime and past-year gambling problems. A future WAGER will address this issue in more detail. Significantly more men than women had at least one problem in the past year in Year 4 and in their lifetimes in Years 1, 4, and 11.
Some limitations of the study noted by Slutske et al. include the sample demographics: a relatively homogenous group of primarily White, Missouri, college students. Perhaps this group had a particularly low incidence of gambling problems because they had little disposable income to spend on gambling or because of the sample selection criteria (i.e. either familial alcoholism or no alcohol problems). Also, they may have had limited access to public gambling opportunities in Missouri over the course of the study. The Missouri State Lottery had only been established the year before the study began, and from 1986-1989, the only legal gambling games available in the state were the lottery and bingo. Only by year 7 (1991), did a riverboat casino open in nearby Illinois.2
Despite these limitations, the study indicates that the lifetime prevalence rates of problem gambling for college students might be lower than previously reported in the literature. This study, like many other prevalence studies, was restricted geographically; the findings from restricted studies might not generalize to the population of college students. National studies of college student gambling and more consistent and reliable measures of past year as well as lifetime problem gambling are necessary to provide better estimates of national prevalence rates.
Comments on this article can be addressed to Michael Stanton at wager@hms.harvard.edu
Notes
1 Sher, K. J., Walitzer, K.S., Wood, P.K. & Brent, E.E. (1991). Characteristics of children of alcoholics:
Putative risk factors, substance use and abuse, and psychopathology. Journal of Abnormal Psychology,
100, 297-308.
2 It is worth noting that by Year 11, additional riverboat casinos were opened in the St. Louis area, the Kansas City area, and the far southeast corner of Missouri, yet the past-year prevalence of problem gambling at Year 11 was at its lowest.
References
*Shaffer, H. J., & Hall, M. N. (2001). Updating and refining meta-analytic prevalence estimates of disordered gambling behavior in the United States and Canada. Canadian Journal of Public Health, 92(3), 168- 172.
**Slutske, W. S., Jackson, K. M., & Sher, K. J. (2003). The natural history of problem gambling from age 18 to 29. Journal of Abnormal Psychology, 112(2), 263- 274.
The WAGER is a public education project of the Division on Addictions at Harvard Medical School. It is funded, in part, by the National Center for Responsible Gaming, the Massachusetts Department of Public Health, the Substance Abuse and Mental Health Services Administration, and the Center for Substance Abuse Treatment.
Copyright ©2003 the President and Fellows of Harvard College