


People with Huntington’s disease1 (HD) often display impulsivity and poor judgment, regardless of their pre-morbid personalities (Stout, Rodawalt, & Siemers, 2001). Parallels might exist between such behavior and research results on frontal lobe2 damage (e.g., Mega & Cummings, 1994) that employs methods to simulate gambling tasks (e.g., Bechara, Damasio, Tranel, & Anderson, 1998). Stout, Rodawalt, and Siemers (2001) suggest that people with HD will show deficits in performance on simulated gambling tasks when compared to patients with Parkinson’s disease3 (PD) and healthy controls.
Stout, Rodawalt, and Siemers (2001) recruited sixty-nine research participants: fourteen with HD, twenty-two with PD, and thirty-three healthy controls. Each participant was asked to select cards from four separate decks to maximize the profit on $2000 of phony money. With each card selection, participants either won money or both won and lost money. Over the course of the test period, two card decks by design led to a net win and two decks by design led to a net loss.
Data show that mild to moderately demented HD patients are more likely than PD patients and healthy controls to display poor judgment and decision making (Stout, Rodawalt, & Siemers, 2001). Indeed, patients with HD chose significantly fewer cards from financially advantageous decks than healthy control participants throughout the duration of the gambling task. Conversely, despite cognitive impairment similar to the HD group, PD patients show better judgment than HD patients. The PD group performed as successfully (i.e., learned to take increasing numbers of cards from financially advantageous decks) as the healthy comparison group throughout the gambling task (Stout, Rodawalt, & Siemers, 2001).
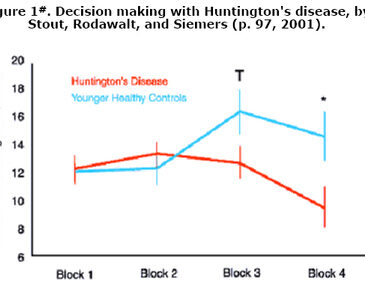
These data indicate that PD and healthy control participants learned over the duration of the gambling task which card decks were most financially advantageous; consequently, they based their selections on this knowledge (Stout, Rodawalt, & Siemers, 2001). While HD patients selected financially disadvantageous cards at similar rates to PD and healthy controls at the beginning of the gambling task, this research indicates that HD patients might not have learned which decks were financially beneficial. Alternatively, perhaps HD patients developed this knowledge but continued-impulsively-to make bad (i.e., risky) selections. According to Stout, Rodawalt, and Simmers (2001), ". . .in administering the gambling task, we noted that several participants with HD indicated during the task that one or more of the decks were ‘bad’, yet they continued to make repeated selections from that deck" (p. 98). Figure 1 illustrates the decision making of the HD group versus healthy controls.

# The sum of choices made from advantageous decks over four blocks of twenty-five trials. "T" indicates a statistical trend at the p<.10 level; "*" indicates a significant trend at the p<.05 level (Stout, Rodawalt, & Siemers, 2001).
Stout, Rodawalt, and Siemers (2001) have contributed significantly to how we understand the relationship between Huntington’s and Parkinson’s disease and risky decision making. However, their work also encourages some questions. The research sample is small; individual subgroups (i.e., HD, PD, and healthy control groups) are even smaller. Do the research results reflect a trend relevant only to this research sample, or do results generalize to diagnostically similar populations? In addition, the results do not indicate whether HD patients are indeed risk-takers. Their propensity to make disadvantageous card selections might be a product of risky decision making, but disadvantageous card selection might also be a product of learning and concept formation disabilities that can accompany HD. Future research should address these uncertainties. Nevertheless, the work of Stout, Rodawalt, and Siemers (2001) should be recognized not only for its contribution to the medical literature on HD and PD, but for its methodological use of gambling tasks as diagnostic tools to measure medical problems.
1 Huntington’s Disease is a hereditary disease of the central nervous system, beginning usually in middle age and characterized by involuntary jerky movements, personality changes, and progressive mental deterioration. It is caused by a mutated gene on chromosome 4. The child of a person with Huntington’s has a 50% chance of inheriting the gene, which inevitably leads to the disease (The Concise Columbia Electronic Encyclopedia, 1999).
2 The frontal lobes are the largest and most anterior part of each cerebral hemisphere (The American Heritage Dictionary of the English Language, Fourth Edition, 2001).
3 A group of Parkinson’s patients was studied because Parkinson’s disease, like Huntington’s, ". . .is associated with preferential damage at a subcortical level of the frontal-striatal brain circuits" (Stout, Rodawalt, & Siemers, 2001, p. 93).
References
Bechara, A., Damasio, H., Tranel, D., & Anderson, S. W. (1998). Dissociation of working memory from decision making within the human prefrontal cortex. Journal of Neuroscience, 18, 428-437.
Mega, M. S., & Cummings, J. L. (1994). Frontal-subcortial circuits and neuropsychiatric disorders. Journal of Neuropsychiatry and Clinical Neurosciences, 6, 38-70.
Stout, J. C., Rodawalt, W. C., & Siemers, E. R. (2001). Risky decision making in Huntington’s disease. Journal of the International Neurological Society, 7, 92-101.
The American Heritage Dictionary of the English Language (4th Edition)(2001). Houghton Mifflin Company. Available: http://www.eref-trade.hmco.com/
The Concise Columbia Electronic Encyclopedia (1999). Columbia University Press. Available: http://www.cc.columbia.edu/cu/cup/
The WAGER is a public education project of the Division on Addictions at Harvard Medical
School. It is funded, in part, by the National Center for Responsible Gaming, the
Massachusetts Department of Public Health, the Addiction Technology Transfer Center of
New England, the Substance Abuse and Mental Health Services Administration, and the
Center for Substance Abuse Treatment.