


There are a variety of treatments used to encourage smokers to stop smoking. However, despite the treatment options, many smokers still struggle to quit (Center for Disease Control and Prevention, 1999). Perhaps smoking cessation treatment could benefit by expanding the variety of treatments available; a particularly novel intervention is Virtual Reality (VR) treatment (Baumann & Sayette, 2006; Carter, Bordnick, Traylor, Day, & Paris, 2008). This week the ASHES reviews a study of the benefits of VR in combination with psychosocial treatment to reduce cigarette smoking (Girard, Turcotte, Bouchard, & Girard, 2009).
Methods
- Researchers recruited 91 healthy adults, aged 18-65, from Quebec, Canada via local ads. Participants were not interested in quitting and smoked ≥10 cigarettes per day.
- Researchers provided participants with brief psychosocial treatment and randomly assigned participants to either experimental (i.e., crushing cigarettes; n = 46) or control (i.e., crushing balls, n = 45) VR sessions.
-
- Clinic visits (weeks 1, 2, 3, 4, 6, 8, 10 and 12): During each 30-minute session, a nurse collected each participant’s smoking journal; performed a carbon monoxide test to confirm abstinence; administered a revised version of the Fagerström test (Heatherton, Kozlowski, Frecker, & Fagerström, 1991) for nicotine dependence (only at weeks 1, 4, and 12); and conducted a brief counseling session.
-
- VR sessions (weeks 1, 2, 3 and 4): Additional 30-minute sessions during which participants in each condition repeatedly simulated grasping the assigned object or crushing it.
- The researchers used an intent-to-treat analysis to analyze all the participants’ results regardless of treatment drop out.
Results
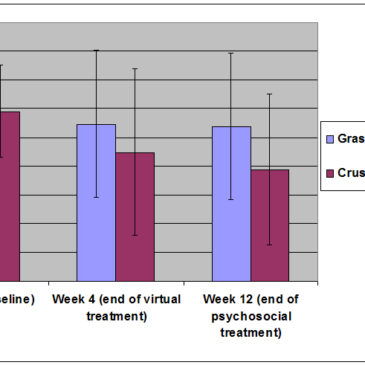
- Researchers tested the program’s impact on the Fagerström test using a repeated measures ANOVA. Figure 1 shows, a significant group (grasping ball or crushing cigarette ) by time (Pretreatment, End of VR, End of program) interaction F (2, 178) = 3.75, p < 0.05.
-
- Contrast analysis revealed that the Cigarette condition was statistically better than the Ball condition at reducing nicotine dependence between week 4, F (1, 89) = 33.34, p < 0.001, and the end of the study F (1, 89) = 55.18, p < 0.001.
- At week 4, there was no significant difference for abstinence between the Ball condition (2%) and the Cigarette condition (9%) (Χ² (1) = 1.84, ns). However, the difference was significant at week 12 between the Ball condition (2%) and the Cigarette condition (15%) (Χ² (1) = 4.79, p < 0.05).
- On average, participants in the Ball condition dropped out of the study significantly earlier than participants in Cigarettes condition (5.89 weeks completed, SD = 4.66; 8.26 weeks, SD = 4.17; respectively; t(89) = 2.56, p < 0.05).

Figure. Fagerström test for Nicotine Dependence. Click image to enlarge.
*Total number of nicotine dependent behaviors (six items) endorsed for a total score between 0 (minimum dependence) and 10 (maximum dependence).
Limitations
- The control group had a higher drop-out rate and, thusly, a greater proportion of early final ratings. Without information on the tendency of drop-outs to show greater or less improvement than completers, it is not possible to gauge the extent to which the outcomes were affected by the intent-to-treat procedure.
- The study uses self-report for some of its measures.
- The study does not explore why crushing cigarettes was more effective than grasping balls for smoking cessation.
Discussion
Compared to the control group, participants whose treatment included crushing cigarettes in a VR environment had lower rates of nicotine dependence, higher cessation rates, and were more likely to remain in the treatment program. What remains illusive about these results is why crushing cigarettes in a VR environment helped participants improve. Future studies should analyze the mechanisms that moderate and mediate these outcomes (e.g., the objective or goal of the treatment session or the subjective states stimulated by crushing cigarettes) utilized in VR. However, these results indicate that VR, combined with more traditional treatment programs, can influence treatment outcomes favorably. Mental health professionals might consider adapting their current treatment programs to include a controlled VR environment.
-Tasha Chandler
References
Baumann, S. B., & Sayette, M. A. (2006). Smoking cues in a virtual world provoke craving in cigarette smokers. Psychology of Addictive Behavior, 20(4), 484-489.
Carter, B. L., Bordnick, P., Traylor, A., Day, S. X., & Paris, M. (2008). Location and longing: The nicotine craving experience in virtual reality. Drug and Alcohol Dependence, 95(1-2), 73-80.
Center for Disease Control and Prevention. (1999). Cigarette smoking among adults: United States. Morbidity & Mortality Weekly Report, 48, 993-996.
Girard, B., Turcotte, V., Bouchard, S., & Girard, B. (2009). Crushing virtual cigarettes reduces tobacco addiction and treatment discontinuation. Cyberpsychology & Behavior, 12(5), 477-483.
Heatherton, T. F., Kozlowski, L. T., Frecker, R. C., & Fagerström, K.-O. (1991). The Fagerström Test for Nicotine Dependence: A revision of the Fagerström Tolerance Questionnaire. British Journal of Addiction, 86(9), 1119-1127.
What do you think? Please use the comment link below to provide feedback on this article.