


Past studies have reported contradictory results regarding the association between tobacco use and risk of suicide (Hemmingsson & Kriebel, 2003; Li, Yang, Ge et al., 2012; Miller, Hemenway, & Rimm, 2000). However, small sample sizes due to the rarity of suicide, and possible unaccounted confounders such as psychiatric illness have limited many of these studies. This week’s ASHES reviews at a study that examines this association within a very large Veterans Health Administration (VHA) sample (Bohnert, Ilgen, McCarthy et al., 2014).
Methods
- Researchers identified patients who used VHA services in financial year (FY) 2005 and were alive in the following year (n=4,863,086)
- Researchers assessed current tobacco use disorder (TUD) status (assessed in FY 2005) and psychiatric illness via the VHA National Patient Care Database
- Researchers determined the cause of all deaths within a 3-year follow-up interval using the Centers for Disease Control and Prevention’s National Death Index
- Researchers created 3 models to investigate the association between tobacco use and suicide mortality
Results
- A larger percentage of patients who qualified for current TUD died by suicide when compared to those who did not qualify for TUD (0.16% vs 0.09%).
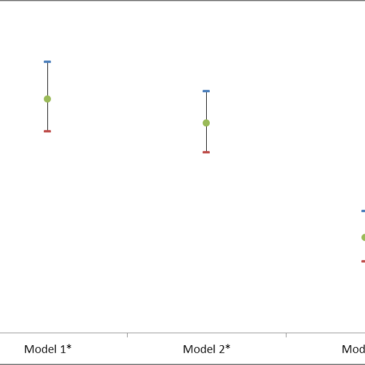
- Figure 1 depicts suicide risk for participants with TUD, compared to those without.
- In Model 1 (unadjusted), having a TUD was significantly associated with an increased risk of suicide (Hazard Ratio (HR) = 1.88, 95% Confidence Interval (CI) = [1.76, 2.02]).
- In Model 2 (adjusted for demographics, general comorbidity, and disability) TUD was similarly associated with increased suicide risk (HR = 1.79, 95% CI = [1.68, 1.91]).
- In Model 3 (adjusted for specific psychiatric conditions) the association was diminished, but remained statistically significant (HR = 1.36, 95% CI = [1.27, 1.46])
")
Figure. Hazard ratios (circular dot) with 95% confidence intervals (black lines) for tobacco use disorder subjects compared to subjects without current tobacco use disorder. (Adapted from Bohnert et al., * p<0.0001). Click image to enlarge.
Limitations
- The VHA sample, which consists predominantly of older male veterans, is not representative of the general population; therefore, one must be cautious when interpreting the results.
- The study does not provide definitive insight into whether the relationships between tobacco use disorder and suicide are causal.
- The reliability of the VHA diagnoses is uncertain. It is possible that assessment of TUD and psychiatric illnesses could be incomplete.
Conclusions
This study reports that tobacco use disorder is associated with increased suicide mortality. The reduced association between TUD and suicide when accounting for specific psychiatric illness suggest that co-occurring psychopathology could partially explain TUD’s association with suicide mortality. However, the fact that the association is still statistically significant suggests that psychiatric illness does not fully explain the association between TUD and suicide mortality. As the study is unable to shed light on any causal aspects of this association, further study is required to determine why TUD and suicide are related.
— Jed Jeng
References
Bohnert, K. M., Ilgen, M. A., McCarthy, J. F., Ignacio, R. V., Blow, F. C., & Katz, I. R. (2014). Tobacco use disorder and the risk of suicide mortality. Addiction, 109(1), 155-162.
Hemmingsson, T., & Kriebel, D. (2003). Smoking at age 18-20 and suicide during 26 years of follow-up — how can the association be explained? International Journal of Epidemiology, 32(6), 1000-1004.
Li, D., Yang, X., Ge, Z., Hau, Y., Want, Q., Liu, F., et al. (2012). Cigarette smoking and risk of completed suicide: a meta-analysis of prospective cohort studies. J Psychiatr Res, 46(10), 1257-1266.
Miller, M., Hemenway, D., & Rimm, E. (2000). Cigarettes and suicide: a prospective study of 50,000 men. Am J Public Health, 90(5), 768-773.
What do you think? Please use the comment link below to provide feedback on this article.
________________
1Charlson comorbidity score: an established measure that classifies comorbidity according to severity
2Adjusted for substance use disorder, PTSD, bipolar disorder, depression, anxiety disorders, and schizophrenia