


Recovery capital refers to internal and external resources an individual can access to start and sustain recovery from a substance use disorder. Social recovery capital — familial, intimate, and social relationships that are supportive of recovery — is one aspect of this. An individual’s personal social network (PSN) and the people within this network (i.e., alters) can influence social recovery capital and impact the ability to maintain abstinence. This week, STASH reviews a study by Meredith W. Francis that investigated differences in the recovery networks of women in treatment for a substance use disorder and whether these impact abstinence outcomes.
What were the research questions?
What kinds of PSNs do women in early recovery from a substance use disorder have, and are they stable over time? What experiences shape these women’s PSNs? Are PSNs associated with the ability to maintain abstinence 12 months after entering treatment?
What did the researcher do?
The researcher analyzed secondary data collected from 377 women enrolled in residential or intensive outpatient substance use disorder treatment in a midwestern U.S. city. Participants reported on their PSN and substance use at four time points: twice during treatment (one week and one month after intake) and twice after treatment (at 6 months and 12 months). Participants also reported on the extent of their trauma symptoms, treatment type, co-occurring disorders, and other experiences.
Three distinct types of recovery networks were identified through a latent profile analysis. Latent transition analyses were used to track movement of participants across PSN types between baseline and 6 months and between 6 and 12 months.
What did they find?
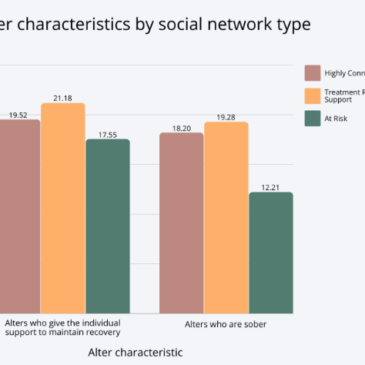
Three kinds of PSNs emerged: Highly Connected (14.3%), Treatment Related Sobriety Support (49.3%), and At Risk (36.3%). Women with Highly Connected networks had tight-knit networks with sober, sobriety-supporting alters and fewer treatment-related alters and isolates. On the other hand, women with Treatment Related Sobriety Support networks also had more sober alters and sobriety supports, but had looser-knit networks with more isolates and treatment-related alters. Finally, women in the At Risk group had less sobriety support, more isolates, fewer sober or treatment-related alters, and more alters with whom they had used (see Figure). Higher trauma symptomatology predicted initial membership in the At Risk typology.
Most of the changes in PSNs happened between 1 week after intake and 6 months, during which 41.6% of women changed their PSN type.1 At 6 months, the majority of women were in the Treatment Related Sobriety Support typology (61.6%), followed by Highly Connected (25.6%) and At Risk (12.8%) typologies. Women with Treatment Related Sobriety Support PSNs were twice as likely to maintain abstinence over the first year compared to those with At Risk PSNs. Interestingly, there were no differences in abstinence rates between the Highly Connected and At Risk groups. Women with a co-occurring disorder were less likely to maintain abstinence, regardless of PSN.
 Figure")
Figure. The mean number of alters (0-25) in each type of social network who give the individual support to maintain sobriety and who are sober. Click image to enlarge.
Why do these findings matter?
Identifying an individual’s PSN at entry to treatment might help predict changes in social networks and treatment outcomes during the first year of recovery, allowing clinicians to target interventions accordingly. For example, women with an At Risk type of PSN generally have less sobriety support. Clinicians could assess their support needs, help identify and link to potential sources of support, and assist in developing relationship-building skills. Because most women transition between PSN typologies in the first 6 months of treatment, clinicians might prioritize the strengthening of recovery networks during this time. Further, these findings reinforce that women with co-occurring disorders and those who have experienced trauma may need additional support during recovery.
Every study has limitations. What are the limitations of this study?
Abstinence was the only outcome variable used to measure recovery, which may not fully capture the nuances of women’s early recovery in relation to their social networks.
For more information:
Are you worried that you or someone you know has an addiction? The SAMHSA National Helpline is a free treatment and information service available 24/7. For more details about addiction, visit our Addiction Resources page.
— Kira Landauer, MPH
What do you think? Please use the comment link below to provide feedback on this article.
________________
[1] Between baseline and 6 months, 41.6% of women changed their PSN typology, 37.1% remained with the same PSN typology, and 21.2% were lost to attrition.