


Today’s review is part of our month-long Special Series on Community Approaches to Addiction. During this Special Series, The BASIS features innovative, community-based addiction interventions that are delivered outside the doctor’s office.
Despite the fact that there are many known risk factors for problem gambling, screening for gambling problems is still not common practice. Though initiatives to promote screening for problem gambling are important and necessary, it is also critical to gather more information regarding what treatment providers actually need to be able to make this change. This week, as a part of our Special Series on Community Approaches to Addiction, The WAGER reviews an article by Sara Guilcher and her colleagues that used concept mapping to assess what social service and healthcare providers need to make screening for problem gambling a part of their regular practice.
What was the research question?
What support and resources do healthcare and social service providers need in order to be able to regularly screen their patients for problem gambling?
What did the researchers do?
With the help of 30 healthcare and service providers (e.g., social workers, case workers, physicians, nurses, psychotherapists), Guilcher and colleagues used concept mapping to understand what changes need to be implemented in order for screening for problem gambling to become everyday practice. Each participant generated answers on their own to the following statement: “If you were directed to routinely screen for problem gambling, what would help you do this in your daily practice?” After all responses were submitted, the researchers sent the participants a list of all of the statements and asked them to group the statements by concept. Participants also ranked each statement by importance and feasibility to implement. With all of this data, researchers created a visual concept map depicting the clusters and statements within each cluster. Finally, the researchers created a “go-zone diagram,” with a go-zone representing all the statements rated above the midpoint of the scale for importance and feasibility/realism.
What did they find?
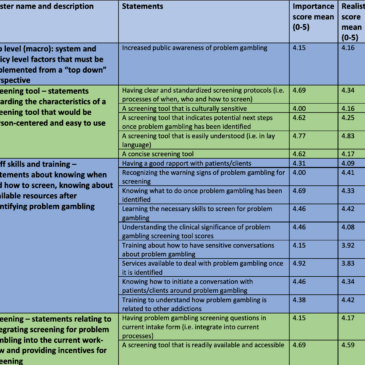
Initially, participants provided 45 unique answers to the prompt. Participants decided after group discussion that a map with the following five clusters best fit the data: (1) top level (i.e., system and policy level factors that need to be implemented from the “top-down,” like community awareness of problem gambling and organizations mandating the screening of problem gambling, (2) characteristics of the screening tool itself, including whether it is culturally sensitive and easy to use, (3) staff skills and training, (4) the screening process (i.e., how to integrate into it into the current workflow; screening incentives) and (5) team resources and support (e.g., minimizing screening burden, having dedicated time for screening, obtaining buy-in from managers). The statement rated most important to implement was, “Services available to deal with problem gambling once it’s identified” and the statement rated most realistic to implement was, “A screening tool that is easily understood (i.e. in lay language)”. The statement, “A problem gambling specialist/expert in-house to screen” was rated as the least important and the least realistic to implement. As the Table shows, the go-zone mostly included statements about staff skills and training and the screening tool itself.
 Image")
Figure. The above table displays the statements in the go-zone by category. Also shown are the statements average ratings of importance and feasibility to implement. The category “Team Resources and Support” had no statements in the go-zone. Table is adapted from Guilcher et al. (2019). Click image to enlarge.
Why do these findings matter?
Most people experiencing problem gambling are not identified or treated for this condition. Screening can identify these cases and help prevent people from developing full-blown Gambling Disorder. This study’s findings have important implications for both treatment providers and policy makers who want to help make screening for problem gambling regular practice, both inside and outside the doctor’s office. The statements listed as most important and feasible provide a good starting place of initial steps that can be taken in order to achieve this goal. These opinions are especially important because they came directly from treatment providers who are the ones interacting with patients and conducting screenings.
Every study has limitations. What are the limitations of this study?
The sample size for the study was small, and only two out of the thirty treatment providers were physicians. Physicians would likely conduct a lot of routine screening for gambling problems, thus it would have been beneficial if they were more represented in the sample. In addition, researchers only sampled treatment providers from a few different hospitals in the Greater Toronto Area, so the results are not generalizable to all healthcare settings.
For more information:
Do you think you or someone you know has a gambling problem? Visit the National Council on Problem Gambling for screening tools and resources. For additional resources, including gambling and self-help tools, please feel free to visit The BASIS Addiction Resources page.
— Alessandra Grossman
What do you think? Please use the comment link below to provide feedback on this article.