


As a group, gay, lesbian, and bisexual (GLB) individuals are more likely to suffer from alcohol use disorders than heterosexual individuals. They also use treatment services for alcohol use disorders at a higher rate than heterosexual individuals. What is not known, however, is whether GLB individuals are more likely than heterosexual individuals to use or gravitate towards one kind of treatment service over another (e.g., private therapists rather than clergy), or if GLB individuals experience additional barriers that might steer them away from treatment services in general. This week, as part of our Special Series on Addiction among the LGBTQ+ Community, The DRAM reviews a study by Junior L. Allen and Orion Mowbray that examines differences in GLB and heterosexual individuals’ use of alcohol treatment services and reasons for not using services.
What was the research question?
Do gay, lesbian, and bisexual individuals give different reasons from heterosexual individuals for not going to alcohol treatment programs?
What did the researchers do?
Allen and Mowbray used data from Waves 1 and 2 of the National Epidemiologic Survey on Alcohol Related Conditions (NESARC). As a part of the survey, participants responded to items related to sexual identity, socio-economic status and demographics, any history of drug use/abuse, any history of mood disorders, use of 15 different alcohol use disorder (AUD) treatment services, and experiences with 26 different barriers to AUD treatment. The participants also completed a DSM-IV-based screen for AUD. The researchers used logistic regression to examine possible associations between sexual orientation (heterosexual: n = 10,874, gay/lesbian: n = 182, bisexual: n = 126) and use of any of the 15 AUD treatment services. Then, limiting their analyses to those who screened positive for lifetime AUD, they used logistic regression to examine possible associations between sexual orientation (heterosexual: n = 1,112, gay/lesbian: n = 31, bisexual: n = 22) and the 26 barriers to treatment.
What did they find?
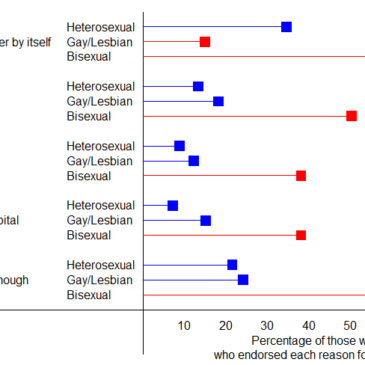
Both the gay/lesbian and bisexual groups had higher rates of alcohol use disorder than heterosexuals. Among all groups, only a fraction of those with AUDs used treatment services: 24.1% of gays and lesbians, 13.9% of heterosexuals, and 29.3% of bisexuals. The difference between heterosexuals and bisexuals was statistically significant. Gay and lesbian individuals were not more likely than heterosexuals to endorse any of the reasons for not seeking treatment; in fact, they were less likely than heterosexuals to believe their problem would go away by itself. Bisexuals were significantly more likely than heterosexuals to endorse many different reasons for not going to treatment (see Figure), including not thinking anyone could help, being afraid of what bosses, friends and family might think, thinking their problem was not serious enough or would go away on its own, and being afraid of being put in a hospital.

Figure. Percentages of NESARC respondents with lifetime AUD who reported different reasons for not seeking treatment. This graphic shows five of the twenty-six reasons for not seeking treatment listed in the study. Lines in red represent percentages of the gay/lesbian or bisexual individuals that were significantly different from the corresponding percentages of the heterosexual individuals. Adapted from Allen and Mowbray (2016). Click image to enlarge.
Why do these findings matter?
One of the purposes of outreach and awareness campaigns is to persuade those who do suffer to seek help. With the additional barriers to treatment that bisexual individuals face, those designing awareness campaigns to reach out to these individuals or communities should consider addressing these specific issues and barriers. For example, they can emphasize that despite what some of them might believe, talking with the right people can help someone overcome alcohol use disorder. Studies that explore differences in subpopulations, like this one, are important. They help the research and treatment communities reach and serve groups that may not connect with more mainstream outreach and awareness programs.
Every study has limitations. What are the limitations in this study?
The list of barriers to treatment might not have been exhaustive enough, and other barriers to treatment might have gone unsaid or undetected. Because the sample sizes of the gay/lesbian and bisexual subgroups were relatively small, some differences in choice of treatment or barriers to treatment might have gone undetected. A similar study with larger subgroups might yield more findings or more definitive results.
For more information:
The Substance Abuse and Mental Health Services Administration (SAMHSA) has a web page dedicated to research and programs designed to serve the LGBT community.
— Matthew A. Tom
What do you think? Please use the comment link below to provide feedback on this article.
Kacy June 29, 2017
Thanks for this very informative post.