


Across addictive behaviors, there is one association that is consistently observed, across studies, methodologies, and samples: substance use at an early age is associated with later problems. Age of onset is one of the best predictors of substance use problems and disorders. We often assume, based on this association, that delaying age of onset ought to reduce the rate of substance use disorders. This week’s edition of The DRAM reviews a study by Ystrom and colleagues (2014) that suggests otherwise for alcohol use.
Methods
- The researchers used data from a study that surveyed members of the Norwegian Institute of Public Health Twin Panel (NIPHTP), a sample representing 63% of the twins born in Norway between 1967 and 1979.
- 638 monozygotic (MZ) twin pairs and 692 dizygotic (DZ) twin pairs participated in the study.
- At the time of the study, most participants were in their twenties, with a mean age of 28.7.
- Measures used in the current study included
- Self-report of age at which participants first drank enough alcohol to feel its influence
- Alcohol use disorder (AUD), as measured by a combination1 of:
- The Composite International Diagnostic Interview (CIDI) assessment for alcohol abuse.
- The CIDI assessment for alcohol dependence
- Current frequency of binge drinking;
- Self-report of having consumed too much alcohol at times.
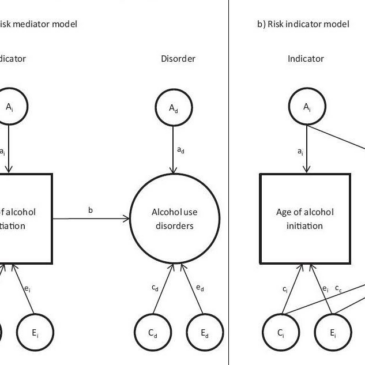
- The researchers tested two models against each other. The causal model suggests that age of initial alcohol use directly influences the development of AUD (as shown in the first panel of Figure 1). On the other hand, the risk indicator model suggests that age of initial use simply reflects underlying genetic and environmental vulnerability which independently increase risk for AUD (as shown in the second panel of Figure 1).
- By using MZ and DZ twins, the researchers were able to assess the amount of variance in their models attributable to genetic factors (represented as “a”), shared environmental factors (represented as “c”), and unique environmental factors (represented as “e”). See ACE Model for more information about these designs.

Figure 1. Theoretical ACE twin study models for the relationship between age of alcohol use initiation and lifetime alcohol use disorder (reprinted from Ystrom et al., 2014). Click to enlarge.
Note. In the causal risk mediator model, early age of alcohol initiation directly influences the development of alcohol use disorder. In the risk indicator model, underlying genetic and environmental factors cause both early age of initiation and alcohol use disorder, but there is no direct causal link between age of initiation and disorder. A = genetic effects; C = shared environmental effects; E = unique environmental effects.
Results
- Overall, the risk indicator model fit the data better than the causal model (Akaike’s information criterion [AIC] = -2.9 and -1.0, respectively).
- The best-fitting risk indicator model, depicted in Figure 2, indicates that:
- approximately 37%2 of the variance in age of first alcohol onset was hereditary in this sample;
- The researcher were able to explain 62%3 of the variance in alcohol use disorder on the basis of hereditary factors. A large proportion (27%) of this variance was shared with the genetic influences on age of first alcohol use, while 35% was unique.

Figure 2. Best-fitting ACE twin study model for the relationship between age of alcohol use initiation and lifetime alcohol use disorder (reprinted from Ystrom et al., 2014).
A = genetic effects; C = shared environmental effects; E = unique environmental effects.
Limitations
- The study was retrospective, meaning that participants had to remember when they had their first drink and what AUD symptoms they had experienced. This introduces the possibility of recall error and bias.
- The study took place in Norway, where the drinking age is lower than the US. That difference and others between the countries could bring the generalizability of the results into question.
Conclusions
The results of this study suggest that age of onset of drinking is a strong marker for AUD risk, but not a cause. In other words, people at risk for the development of AUD due to genetic and environmental risk factors are also likely to begin drinking earlier, but this early drinking does not itself contribute substantially to the development of AUD. This suggests that preventing early drinking is unlikely to prevent AUD among these at-risk individuals. Early substance use has many other negative consequences, including irreversible effects on the developing brain, so this study should not be taken as grounds to cease prevention efforts. Instead, the findings suggest that intervention efforts need to also identify and focus on those modifiable risk factors that influence both early alcohol use and the development of AUD.
– Sarah Nelson
What do you think? Please use the comment link below to provide feedback on this article.
References
Ystrom, E., Kendler, K. S., & Reichborn-Kjennerud, T. (2014). Early age of alcohol initiation is not the cause of alcohol use disorders in adulthood, but is a major indicator of genetic risk. A population-based twin study. Addiction, 109, 1824-1832.
Notes
1 To combine the measures of AUD, the researchers conducted a confirmatory factor analysis and then included the latent AUD construct in other models.
2 Wondering where this number comes from? It derives from the path-coefficient in Figure 2 representing genetic influence on age at alcohol initiation. We square this value – 0.61—in order to estimate the proportion of variance in age of alcohol initiation explained by genetic risk factors.
3 For this number, we sum the squares of the two genetic path-coefficients leading to alcohol use disorder in Figure 2 (i.e., -0.522 + 0.612).