


Drug use and misuse of prescription drugs is an important condition (Cherpitel & Ye, 2008) often unrecognized by primary care physicians (Saitz, Mulvey, Plough, & Samet, 1997) who might be compromised by the limited amount of time they can devote to each patient. Research indicates that brief screening instruments might help physicians identify patients with concomitant conditions as diverse as gambling-related disorders (Gebauer, LaBrie, & Shaffer, 2010) and misuse of prescription medications (Humeniuk, Dennington, & Ali, 2008; Madras et al., 2009). This week the STASH reviews the report of a study testing the utility of a single drug use screening question for use within primary care offices (Smith, Schmidt, Allensworth-Davies, & Saitz, 2010).
Methods
- Participants (n=286; 62.6% Black/African American, 17.1% White, 16.1% Hispanic /Latino ethnicity, 4.2% other) were randomly recruited from a primary care office that primarily serves uninsured low-income patients.
- Of the 1,781 people approached, 903 agreed to screening and 394 of these were eligible for the study (i.e. they were clinic patients at least 18 years old, able to complete the questionnaires in English, and free of acute illness). Participants who consented, had no lost data, and completed the study were included in the analysis.
- Trained interviewers administered the single question screen for drug use (i.e., “How many times in the past year have you used an illegal drug or used a prescription medication for nonmedical reasons?”).1
- The researchers explored the single-item screen’s sensitivity and specificity with regard to current (past 12 months) self-reported illicit drug use (i.e., illicit drugs included misuse of prescription drugs) and current drug use disorders. The researchers measured disordered drug use using a computerized version of the Composite International Diagnostic Interview (CIDI) Substance Abuse Module2.
- After the interview participants were asked to participate in an oral fluid test (i.e., a saliva drug test). A total of 217 participants (76%) consented to provide saliva and indicated whether they had a recent prescription for opiates or benzodiazepines. Positive test results for drugs with prescribed current use were not considered to indicate illicit use.
- The researchers compared the sensitivity and specificity of the single question drug use screen to identify patients with a current self-reported illicit drug use and current drug use disorder (measured using the CIDI) to a longer (i.e., 10-item) screen that research indicates is a valid and reliable measure of drug abuse: the DAST-10 (Yudko, Lozhkina, & Fouts, 2007).
Results
- The prevalence rate was 34.6% (n = 99) for self-reported current drug use and 12.9% (n = 37) for current drug abuse (n = 3) or drug dependence (n = 34). Among the 217 participants who consented to oral fluid testing, 18.3% (n = 44) had a positive oral fluid test result.
- The 44 participants with positive biological results included 11 (25%) who denied during the interview that they used drugs.
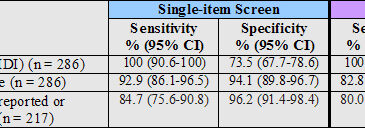
- As Tables 1 shows, the single-item screen was similar to the DAST-10 for the detection of current drug use disorders and current self-reported drug use.

Figure. Sensitivity and specificity detection of the single-item screen and the DAST-10 (adapted from Smith et al., 2010) *CI: Confidence interval. Click image to enlarge.
Limitations
- The single-item screen is a compound question. It is not possible to distinguish which part of the question the respondent is answering (i.e., illegal drugs or prescription medication for nonmedical use).
- The willingness to self-report drug use and drug-related problems was not shared by participants whose denied use was contradicted by a biological test (25% of those tested). The effect on sensitivity is shown in the last row of Table 1 from the report.
- The participants were recruited from a population with a higher prevalence of drug use than the general population. Among a general population with lower base-rates of current drug use and drug use disorders, the single-item screen might yield lower sensitivity and specificity.
Discussion
This single-item screening tool performed similarly to a longer substance use screen and might be well-suited for substance use detection within primary care offices because physicians have a limited amount of time with patients. However, it is important to note the distinction between screens and assessment or diagnostic tools. This screen does not distinguish between patients who might benefit from substance abuse treatment versus those who might benefit from brief interventions while visiting a primary care office, whereas a more in-depth assessment might.
-Tasha Chandler
What do you think? Please use the comment link below to provide feedback on this article.
References
Cherpitel, C. J., & Ye, Y. (2008). Drug use and problem drinking associated with primary care and emergency room utilization in the US general population: Data from the 2005 national alcohol survey. Drug and Alcohol Dependence, 97(3), 226-230.
Gebauer, L., LaBrie, R. A., & Shaffer, H. J. (2010). Optimizing DSM-IV classification accuracy: A brief bio-social screen for detecting current gambling disorders among gamblers in the general household population. Canadian Journal of Psychiatry, 55(2), 82-90.
Humeniuk, R., Dennington, V., & Ali, R. (2008). The effectiveness of a brief intervention for illicit drugs linked to the Alcohol, Smoking and Substance Involvement Screening Test (ASSIST) in primary health care settings: A technical report of Phase III findings of the WHO ASSIST randomized controlled trial. Geneva, Switzerland: World Health Organization.
Madras, B. K., Compton, W. M., Avula, D., Stegbauer, T., Stein, J. B., & Clark, H. W. (2009). Screening, brief interventions, referral to treatment (SBIRT) for illicit drug and alcohol use at multiple healthcare sites: comparison at intake and 6 months later. Drug and Alcohol Dependence, 99(1-3), 280-295.
Saitz, R., Mulvey, K. P., Plough, A., & Samet, J. H. (1997). Physician unawareness of serious substance abuse. The American Journal of Drug and Alcohol Abuse, 23(3), 343-354.
Smith, P. C., Schmidt, S. M., Allensworth-Davies, D., & Saitz, R. (2010). A single-question screening test for drug use in primary care. Archives of Internal Medicine, 170(13), 1155-1160.
Yudko, E., Lozhkina, O., & Fouts, A. (2007). A comprehensive review of the psychometric properties of the Drug Abuse Screening Test. Journal of Substance Abuse Treatment, 32(2), 189-198.
________________
[1]The single-item screen was scored positive if participants answered at least 1 time. If asked to clarify the meaning of “nonmedical reasons,” the research associate added “for instance because of the experience or feeling it caused.” (Smith et al., 2010).
[2]The CIDI is a comprehensive assessment tool that integrates criteria and definitions from the 10th revision of the International Statistical Classification of Diseases and Related Health Problems (ICD-10) and the 4th revision of the Diagnostic and Statistical Manual (DSM-IV).