


The process of screening for addictive behaviors is moving from research labs into the mainstream of public health practice (Anderson, Aromaa, Rosenbloom, & Enos, 2008). Most people and programs that consider administering public health screens face significant temporal and financial restrictions. Consequently, the development of brief screens that can identify the most people in need of treatment, without also generating many false positives, is critical. Among the general population, pathological gambling (PG) is a relatively rare disorder (Kessler et al., 2008; Petry, Stinson, & Grant, 2005). As a result, public health workers tend to screen for and detect PG less often than other more prevalent expressions of addiction, such as alcohol and other drug dependence. Until now, there were only two brief screens for detecting PG among the general population (i.e., the Lie/Bet Questionnaire, and the MAGS 7, respectively; Johnson et al., 1997; Shaffer, LaBrie, Scanlan, & Cummings, 1994). This week the WAGER compares two new, independent and nearly simultaneously published reports focusing on the development of brief screens for PG (Gebauer, LaBrie, & Shaffer, in press; Toce-Gerstein, Gerstein, & Volberg, in press).
Methods
- The Brief Bio-Social Gambling Screen (BBGS; Gebauer et al., in press)
- Gebauer et al. developed the BBGS using past year DSM-IV PG items from the Alcohol Use Disorder and Associated Disabilities Interview Schedule IV (AUDADIS-IV; Grant, Dawson et al., 2003) that was included within the National Epidemiological Survey on Alcohol and Related Conditions (NESARC; Grant, Moore, & Kaplan, 2003).
- The NESARC survey collected information from a United States nationally representative random sample of individuals (N=43,093) from the general household population.
- Gebauer et al. targeted participants who endorsed five or more DSM-IV symptoms or signs as the group of pathological gamblers (PGs) to be distinguished from participants who failed to meet these criteria.
- The researchers used data analytic procedures, including step-wise entry, step-wise elimination, and combinations of minimal sets of DSM-IV criteria, to identify the subset of DSM-IV criteria that was sufficiently sensitive to identify PGs correctly, and specific enough to exclude non-PGs from being incorrectly classified as PGs (i.e., false positives).
- Gebauer et al. developed the BBGS using past year DSM-IV PG items from the Alcohol Use Disorder and Associated Disabilities Interview Schedule IV (AUDADIS-IV; Grant, Dawson et al., 2003) that was included within the National Epidemiological Survey on Alcohol and Related Conditions (NESARC; Grant, Moore, & Kaplan, 2003).
- The NODS-CliP (Toce-Gerstein et al., in press)
- Toce-Gerstein et al. (in press) developed the NODS-CLiP using lifetime DSM-IV PG items from the NORC Diagnostic Screen for Gambling Disorders (NODS; Gerstein et al., 1999).
- Researchers administered the NODS to participants (N=17,180) in eight different general adult population field studies.
- Toce-Gerstein et al. targeted participants who endorsed five or more DSM-IV symptoms or signs as the group of PGs to be distinguished from participants who failed to meet these criteria.
- The researchers developed the NODS-CliP by analyzing how well each possible subset of 2-4 NODS items identified PG.
- Toce-Gerstein et al. (in press) developed the NODS-CLiP using lifetime DSM-IV PG items from the NORC Diagnostic Screen for Gambling Disorders (NODS; Gerstein et al., 1999).
Results
- Both the NODS-CLiP and the BBGS offer three items as a brief screen that can identify PGs from the general population.
- NODS-CLiP
- Loss of Control: Have you ever tried to stop, cut down, or control your gambling?
- Lying: Have you ever lied to family members, friends or others about how much you gamble or how much money you lost on gambling?
- Preoccupation: Have there been periods lasting 2 weeks or longer when you spent a lot of time thinking about your gambling experiences, or planning out future gambling ventures or bets?
- BBGS
- Withdrawal: During the past 12 months, have you become restless, irritable or anxious when trying to stop/cut down on gambling?
- Deceive: During the past 12 months, have you tried to keep your family or friends from knowing how much you gambled?
- Bailout/Need Money: During the past 12 months, did you have such financial trouble that you had to get help with living expenses from family, friends, or welfare?
- NODS-CLiP
- Psychometric Values
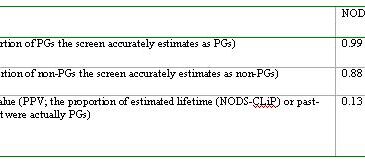
- Table 1 summarizes the psychometric values for both the NODS-CLiP and the BBGS (i.e., Sensitivity, Specificity and Positive Predictive Values).
Table 1. Comparing the Psychometric Values of the NODS-CLiP and the BBGS
 *Click image to enlarge, or adjust your browser's zoom setting.
*Click image to enlarge, or adjust your browser's zoom setting.
Limitations
- The NODS-CliP identified lifetime PG; the BBGS identified past-year PG.
- Using a lifetime context for symptom clustering is problematic. This strategy yields more endorsed problems than past-year time frames for symptom identification; further, using a lifetime frame for screening is inconsistent with the process of making a clinical diagnosis. For example, research shows that gambling related problems evidence considerable waxing and waning from year to year (LaPlante, Nelson, LaBrie, & Shaffer, 2008). As a result, the NODS-CliP might not reflect current problems that often associate with treatment seeking. The BBGS features current problem identification. The different PPVs, in part, reflect this circumstance.
- Because the NODS-CLiP uses a lifetime context for symptom identification, the PGs who screened positive might not present as PGs currently. As a result, the NODS-CLiP’s sensitivity, its apparent strength (i.e., 0.99 for the NODS-CLiP vs. 0.96 for the BBGS), is uncertain for applications seeking to identify current PG.
- Both studies were limited because both teams of researchers selected PG items from those that currently were available in the DSM-IV.
- The DSM-IV criteria do not represent an exhaustive list of sequelae associated with PG and there is no empirical evidence that, despite its reliability, the DSM-IV includes conceptually valid diagnostic criteria. In fact, the efficacy of both screens serves to demonstrate that some of the DSM diagnostic criteria for PG fail to discriminate it adequately from those who do not suffer with this problem.
- Both studies are subject to the problems associated with data obtained exclusively from self-report.
Conclusions
Which screen wins? One clear advantage of the BBGS is the assessment of past year PG, which is consistent with clinical practice, compared to lifetime PG. Beyond this, determining the answer really depends on the goal of screening. For most clinical programs, time and money are precious resources that cannot be wasted. If an agency was to conduct follow-up evaluations with those identified as PGs by the NODS-CLiP, we would expect only one in eight to be identified correctly as a PG; however, of those identified as a PG by the BBGS, approximately one in three would be identified correctly as a PG. A screen that yields many false positives (e.g., 7 for every 8 screened), and does not maximize specificity, is best to garner liberal estimates of problems, but has limited clinical utility. Therefore, for clinical programs, a screen with superior specificity and high sensitivity makes the most sense (i.e., BBGS). Nevertheless, for researchers and others who simply want to identify the most PGs possible, without care for false positives, the slight sensitivity advantage evidenced by the NODS-CLiP might make it more attractive. Ultimately, you will have to decide the goal of screening, and then pick the measure that best achieves that goal.
What do you think? Please use the comment link below to provide feedback on this article.
References
Anderson, P., Aromaa, S., Rosenbloom, D., & Enos, G. (2008). Screening and Brief Intervention: Making a Public Health Difference. Boston: Join Together.
Gebauer, L., LaBrie, R. A., & Shaffer, H. J. (in press). Optimizing DSM-IV classification accuracy: A brief bio-social screen for gambling disorders among the general household population. Canadian Journal of Psychiatry.
Gerstein, D., Murphy, S., Toce, M., Hoffmann, J., Palmer, A., Johnson, R., et al. (1999). Gambling Impact and Behavior Study: Report to the National Gambling Impact Study Commission. Chicago: National Opinion Research Center.
Grant, B., Dawson, D., Stinson, F., Chou, P., Kay, W., & Pickering, R. (2003). The Alcohol Use Disorder and Associated Disabilities Interview Schedule-IV (AUDADIS-IV): Reliability of alcohol consumption, tobacco use, family history of depression and psychiatric diagnostic modules in a general population sample. Drug & Alcohol Dependence, 71, 7-16.
Grant, B., Moore, T., & Kaplan, K. (2003). Source and Accuracy Statement: Wave 1 National Epidemiologic Survey on Alcohol and Related Conditions (NESARC). Bethesda, MD: National Institute on Alcohol Abuse and Alcoholism.
Johnson, E. E., Hamer, R., Nora, R. M., Tan, B., Eisenstein, N., & Engelhart, C. (1997). The Lie/Bet Questionnaire for screening pathological gamblers. Psychological Reports, 80, 83-88.
Kessler, R. C., Hwang, I., LaBrie, R. A., Petukhova, M., Sampson, N. A., Winters, K. C., et al. (2008). DSM-IV pathological gambling in the National Comorbidity Survey Replication. Psychological Medicine 38(9), 1351-1360.
LaPlante, D. A., Nelson, S. E., LaBrie, R. A., & Shaffer, H. J. (2008). Stability and progression of disordered gambling: Lessons from longitudinal studies. Canadian Journal of Psychiatry, 53(1), 52-60.
Petry, N. M., Stinson, F. S., & Grant, B. F. (2005). Comorbidity of DSM-IV pathological gambling and other psychiatric disorders: Results from the National Epidemiologic Survey on Alcohol and Related Conditions. Journal of Clinical Psychiatry, 66(5), 564-574.
Shaffer, H. J., LaBrie, R., Scanlan, K. M., & Cummings, T. N. (1994). Pathological gambling among adolescents: Massachusetts gambling screen (MAGS). Journal of Gambling Studies, 10(4), 339-362.
Toce-Gerstein, M., Gerstein, D., & Volberg, R. (in press). The NODS-CLiP: A rapid screen for adult pathological and problem gambling. Journal of Gambling Studies, epub ahead of print.
NADEAU Claude-Henri August 14, 2009
The decisive criteria is PPV. According to PPV, each screen is very weak.
BASIS Staff August 19, 2009
As we mentioned in the WAGER 14(6), positive predictive value (PPV) is one of several psychometric properties, and the purpose for the screening, not the different properties, determines the best fit. Concerning your assertion that the PPV is ‘weak’ for both screens, screens that target low base rate disorders tend to have low PPV’s. The PPV’s for the NODS-CliP and BBGS (i.e., 0.13 and 0.37 for respectively) compare quite favorably with brief screens that target other low base rate phenomena. Donker, van Straten, Marks and Cuijpers (2009) found PPV’s similar to the BBGS for screen of numerous mental health and substance abuse disorders that typically have higher prevalence rates (Kessler, Berglund, Demler, Jin, & Walters, 2005) compared to pathological gambling (e.g., obsessive compulsive disorder, lifetime prevalence=1.6%, PPV=0.15; panic disorder, lifetime prevalence=4.7%, PPV=0.10; generalized anxiety disorder, lifetime prevalence=5.7%, PPV=0.29; post-traumatic stress disorder, lifetime prevalence=6.8%, PPV=0.11; alcohol abuse/dependence, lifetime prevalence=18.6%, PPV=0.34). With a PPV of 0.37, the BBGS represents a meaningful advance in a nascent area of public health.
Donker, T., van Straten, A., Marks, I., & Cuijpers, P. (2009). A brief web-based screening questionnaire for common mental disorders: Development and validation. Journal of Medical Internet Research, 11(3).
Kessler, R. C., Berglund, P., Demler, O., Jin, R., & Walters, E. E. (2005). Lifetime Prevalence and Age-of-Onset Distributions of DSM-IV Disorders in the National Comorbidity Survey Replication. Archives of General Psychiatry, 62(6), 593-602.
Dean Gerstein August 23, 2009
The WAGER’s comparison of the NODS-CLiP with the BBGS, a screen developed by two of its staff members and a colleague, fails to consider the following highly critical issue:
The clinical validity and diagnostic reliability of the NODS, from which the NODS-CLiP is derived and against which it was benchmarked, were established by its authors (of which I am one) prior to fielding the NODS, and these psychometrics have subsequently been confirmed by other researchers on several continents, as cited in the paper by Toce-Gerstein and her colleagues (in press).
In contrast, zero studies have been published on the clinical validity or diagnostic reliability of the AUDASIS-IV gambling module (AGM), from which the BBGS is derived and against which it is benchmarked. The citation authored by Grant, Dawson, and colleagues (2003), which is the cited basis for evaluating the psychometric properties of this benchmark, clearly reports that no clinical validity studies of the AGM were undertaken prior to its deployment in the NESARC, and as to its diagnostic reliability—as opposed to the test-retest reliability of individual items in non-clinical cases—that could not even be estimated because zero cases of pathological gambling (that is, a score of five or more DSM symptoms) showed up in the test-retest sample that Grant and her colleagues report on.
I have other issues with The WAGER’s comparison, but this one huge hole under the BBGS is sufficient to sideline it from entering any purported contest of virtues.
Dean Gerstein August 25, 2009
The WAGER paper ignores one very important matter.
The NODS-CLiP is based on and checked against the NODS. The inventors of the NODS tested its clinical validity and reliability before they used it, and their good test results have been confirmed repeatedly by others, as noted in the cited paper by the Toce-Gerstein team.
The BBGS is taken from and checked against the gambling items in the AUDASIS-IV. Grant and her team are the only ones who have tested these items. Their report clearly says that no study of the validity of these items has been done, and they could not estimate clinical reliability because no cases of pathological gambling showed up in their test/retest study.
There are other problems with THE WAGER paper, but this one huge hole under the BBGS is enough to keep it even from entering the field of “battle.” The NODS-CLiP “wins” by default.
Matt stevens September 27, 2009
One would expect to see differences in psychometrics between the two screens, as the NODS-CLiP measures lifetime, while the BBGS measures last 12 months. There is increasing evidence that the majority of people who develop gambling related problems move in and out of problem gambling episodes and like most “addictions” the majority of people cease the problematic behaviour of their own accord. Sets of lifetime questions will always be more likely to generate false positives because of the more often transient nature of problem gambling. It makes sense to have a single questions relating to lifetime, but not every question in a screen.