


Disasters, such as recent hurricanes and floods in North America, earthquakes in Indonesia, the 2004 tsunami in Southeast Asia, and the New York City World Trade Center attack, have killed thousands and exposed thousands more to ongoing trauma. Survivors probably manage the aftermath of such disasters by utilizing coping methods dependent upon their current situation; specific strategies vary by culture. For example, researchers have found differences in social support and coping among different racial and ethnic groups (Pole et al., 2005; Kim et al., 2007.) This week, Addictions and the Humanities considers whether people exposed to the World Trade Center attack from different racial, ethnic, and cultural backgrounds experienced different addiction-related health outcomes.
Unfortunately, it is difficult to conduct disaster research for a number of reasons. Disasters vary in many ways: geographic size, mortality rates, elapsed time, and displacement among others. Such differences make studying the effect and generalizability of findings related to disasters and their aftermath challenging.
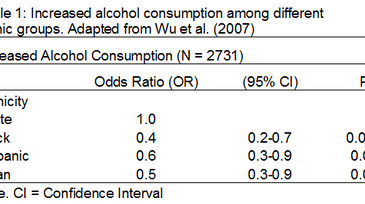
To study the effect of the World Trade Center attack (WTC attack) on increased cigarette and alcohol use, Wu et al. (2006) drew a stratified random sample of all high school students in New York City and had the students complete a survey about their exposure (direct, family or media) and their cigarette and alcohol use after the WTC attack. Researchers examined participants’ self-reports that they “started” or “increased” smoking/drinking after the WTC attack. Analyses revealed that students directly exposed to the attack reported increased alcohol use after the WTC attack, Odds Ratio (OR) 1.8 (95% CI, 1.1-2.8). Researchers compared African Americans, Asian American and Hispanic American students to their non-Hispanic white counter parts; these minority groups were protected from increased alcohol use after the WTC attack. The OR for African American students was 0.4 (95% CI, 0.2-0.7), for Asian American students the OR was 0.5 (95% CI, 0.3-0.9), and for Hispanic American students the OR was 0.6 (95% CI, 0.3-0.9) (see Table 1).

There are several limitations to discuss. The study is not longitudinal; therefore, it is impossible to determine if exposure to the WTC attack precipitated the change in smoking and drinking behavior. Second, the population studied was high school students in New York City. Consequently, the results should only be generalized to adolescents involved in disasters where displacement is minimal, as was the case in NY. Finally, researchers asked only if subjects initiated or increased use of alcohol and cigarettes but not other substances of abuse. This makes it difficult to determine the degree to which substance use increases after a disaster.
The finding that Asian, Hispanic and African-American students drank alcohol less than non-Hispanic whites is interesting and warrants further study. This finding contrasts with results from the Youth Risk Behavior Surveillance System, which identified higher alcohol use prevalence rates among Hispanic and non-Hispanic white students compared to African-American students (Eaton et al., 2006). It is possible that certain cultural values might have lead to protection against alcohol abuse or that certain cultures abuse other substances not measured in response to disasters. Future studies must use comprehensive measures of substance use, focus more on cultural differences, and follow up with students over a longer period of time. Researchers also must study whether coping mechanisms manifest differently in various geographical areas and cultures. If more research identifies cultural coping differences, these results should inform public health strategies and interventions.
What do you think? Comments can be addressed to John Kleschinsky.
References
Eaton, D. K., Kann, L., Kinchen, S., Ross, J., Hawkins, J., Harris, W. A., et al. (2006). Youth risk behavior surveillance–United States, 2005. MMWR Surveillance Summaries, 55(5), 1-108.
Kim, J. H., Knight, B. G., & Longmire, C. V. (2007). The role of familism in stress and coping processes among African American and White dementia caregivers: Effects on mental and physical health. Health Psychology, 26(5), 564-576.
Pole, N., Best, S. R., Metzler, T., & Marmar, C. R. (2005). Why are hispanics at greater risk for PTSD? Cultural Diversity and Ethnic Minority Psychology, 11(2), 144-161.
Wu, P., Duarte, C. S., Mandell, D. J., Fan, B., Liu, X., Fuller, C. J., et al. (2006). Exposure to the World Trade Center attack and the use of cigarettes and alcohol among New York City public high-school students. American Journal of Public Health, 96(5), 804-807.