


The social setting exerts considerable influence on drug using and other behaviors. Acculturation, the process of immigrants and subsequent generations adapting to a new culture while maintaining their prior culture, is important to health behaviors (see, ASHES, Vol. 2(1)). For example, Guevarra at al. (2005) found that in the United States, the more closely African-American women identified to their African-American culture the less likely they were to smoke. Similarly, having immigrant parents in the United States can be a protective factor for smoking (Acevedo-Garcia, Pan, Jun, Osypuk, & Emmons, 2005). Yet, certain ethnic groups, like Asian Americans, report a higher prevalence rate of smoking than the general population (Ma et al., 2005). These research findings demonstrate the complex relationship between acculturation and smoking. This week’s ASHES reports on a study that critically examined ethnic identity and mediating acculturation factors of smoking in Canadian adolescents (Asbridge, Tanner, & Wortley, 2005).
Students (N=3,400) from 30 Toronto high schools completed questionnaires that included measures of ethnic identity and cultural retention. Participants self-identified their ethnicity/ethnicities by choosing from 12 different ethnic groups: Canadian, Western European, Eastern European, Southern European, Chinese, South Asian and East Indian, South-East Asian, West Asian and Middle Eastern, West Indian, Hispanic, African, and other. Questions on ethnic music, language spoken at home, and attendance of cultural/ethnic events measured cultural retention (acculturation to one’s ethnic culture). Participants reported how often they used tobacco in the last year and if their peers and siblings smoked.
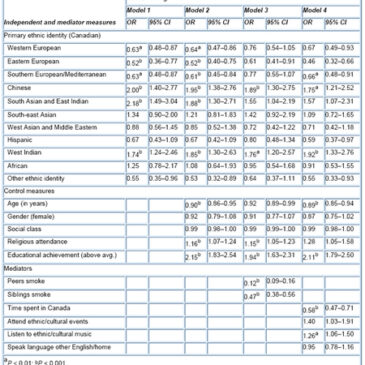
Smoking differences along ethnic lines is attributable, in part, to acculturation factors. The prevalence of non-smokers varied by ethnicity: Chinese (79.9%), South Asian & East Indian (84.1%), West Indian (84.3 %) African (80.9%) Western European (62.5%), Eastern European (57.5%), Southern European (61.7%), and other (57.7%). However, a four-stage multivariate analysis (see Figure) showed that control measures (e.g., age, education, etc.) and mediating factors (e.g., peer smoking, time spent in Canada) might have explained some ethnic differences. Model 1 showed that ethnicity related to non-smoking – the ethnic groups significantly more likely to be smokers were Western, Eastern, and Southern Europeans.; however, model 2 showed that control variables did not change this finding. Furthermore, Models 3 and 4 shows that after adjusting for control variables, peer and sibling smoking and acculturation factors explained non-smoking for some groups. For example, including peer and sibling smoking explained why the Europeans smoked more but it had little or no effect on the non-smoking groups.

Figure. Logistic regression of non-smoking on primary ethnic identity, controls and mediators. Adapted from asbridge et al. (2005). Click image to enlarge.
The study’s cultural retention measure is a study limitation. A robust assessment of acculturation that includes items about both one’s ethnic culture and host culture might provide a more comprehensive analysis of ethnic identity and smoking. The present study only measured one’s identity to their ethnic culture, but did not include items about their Canadian identity, other than time spent in Canada. More studies should comprehensively assess acculturation when examining the relationship between ethnic identity and health risk behaviors like smoking. Another limitation is that the data represents a single point in time; it is instructive to follow youths and determine in real time how different factors mediate their smoking-related decisions. Finally, the study could have examined acculturation changes by grouping age and length of time in Canada. Absent this information, the study was unable to examine how acculturation mediated smoking factors as students grew older and their identities took shape, as that relationship might change.
The present study provides some interesting insight about the interaction between ethnic identity and smoking; however, further research is needed to fully examine this relationship. Not only will these findings help prevention and intervention programs become more culturally competent, but additional research might also promote more awareness and education on high-risk behaviors within ethnic communities, and provide more evidence to guide researchers and public health agencies to better understand the influence of acculturation on a wide array of health behaviors.
–Sarbani Hazra.
References
Acevedo-Garcia, D., Pan, J., Jun, H.-J., Osypuk, T. L., & Emmons, K. M. (2005). The effect of immigrant generation on smoking. Social Science & Medicine, 61(6), 1223-1242.
Asbridge, M., Tanner, J., & Wortley, S. (2005). Ethno-specific patterns of adolescent tobacco use and the mediating role of acculturation, peer smoking, and sibling smoking. Addiction, 100(9), 1340-1351.
Guevarra, J. S., Kwate, N. O. A., Tang, T. S., Valdimarsdottir, H. B., Freeman, H. P., & Bovbjerg, D. H. (2005). Acculturation and Its Relationship to Smoking and Breast Self-Examination Frequency in African American Women. Journal of Behavioral Medicine, 28(2), 191-199.
Ma, G. X., Shive, S. E., Tan, Y., Toubbeh, J. I., Fang, C. Y., & Edwards, R. L. (2005). Tobacco use, secondhand smoke exposure and their related knowledge, attitudes and behaivors among Asian Americans. Addictive Behaviors, 30(4), 725-740.
What do you think? Please use the comment link below to provide feedback on this article.