


Recent research on chemical and behavioral addiction (e.g., alcoholism and gambling) suggests that such seemingly disparate problems might be related. Neuroimaging studies (fMRI) have revealed that the neurological reward pathways associated with psychoactive substance use (e.g., cocaine) overlap with reward pathways associated with non-drug related experiences (e.g., appreciation of beauty or monetary expectations) (Aharon, Etcoff, Ariely, Chabris, O’Connor, & Breiter, 2001; Breiter, Aharon, Kahneman, Dale, & Shizgal, 2001). Increasingly, researchers are turning their attention to eating disorders, such as binge eating, to see whether these reward system similarities also apply to this area of excess. Recognizing the frequent co-occurrence of binge eating and alcohol disorders, Kane,
Loxton, Staiger, and Dawe (2004) investigated whether these disorders shared an impulsivity link. This week The DRAM reviews the results of their study.
Kane et al. (2004) recruited 66 women to participate in this study: 23 met DSM criteria for both bulimia nervosa and alcohol abuse or dependence (i.e., the comorbid group); 22 met criteria for bulimia only (i.e., the bulimia group); and 21 met criteria for neither disorder (i.e., the control group). Study participants completed five questionnaires related to alcohol use, eating disorders, anxiety, and impulsivity, as well as a behavioral impulsivity measure, the Card Arranging Reward Responsiveness Objective Test (CARROT — Powell, Al-Adawi, Morgan, & Greenwood, 1996). The CARROT is used to test motivation by measuring the speed at which participants perform a card-sorting task after learning of an incentive to complete it, such as a small financial reward. A recent study found that CARROT scores (i.e., the change in speed of task-completion when presented with the possibility of a reward) significantly increased in heavy-drinking college students after being exposed to the sight, smell, and/or taste of alcohol (Kambouropoulos & Staiger, 2001).

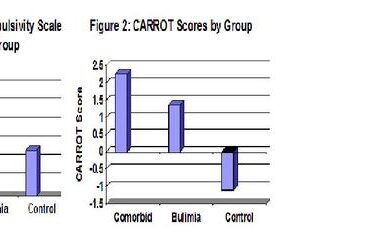
Figures 1 and 2. Comparing impulsivity across comorbidity, bulimia and control groups (adapted from Kane et al., 2004). Click image to enlarge.
Figures 1 and 2 illustrate the average impulsivity response for each group, for each of the two impulsivity measures. Both the Eysenck Scale (Eysenck & Eysenck, 1991; Fabian, 1990) and the CARROT measures were significantly different across the participant groups, F(2, 63)=17.13, p<0.001 and F(2, 63)=3.17, p<0.05, respectively. Similarly, on the Eysenck scales, each of the study groups was significantly different from the other two groups. On the CARROT tests, each of the bulimic groups was significantly different from the control group but, in part because of the small sample size, the bulimic groups were not significantly different from each other. In both instances, the comorbid group evidenced more impulsivity than the bulimia only group; in turn, the bulimia only groups reported
more impulsivity than the control groups.
This study would benefit from larger sample sizes and a more diverse study population; it also would be important to add an alcohol-only problem group for comparison. It would be interesting to gain a better understanding of how impulsivity influences the development of disordered eating and drinking, but due to the cross-sectional design of this study it was not possible to distinguish causal relationships.
This research draws attention to an important common factor between chemical and behavior expressions of excessive behavior. The results demonstrate relationships of both impulsivity and motivation to work for a reward with the presence of bulimia as well as bulimia and comorbid disordered drinking. Both factors could be important in understanding the development of these disorders and designing therapies to treat bulimia and bulimia that cooccurs with an alcohol use disorder.
What do you think? Please use the comment link below to provide feedback on this article.
References
Aharon, I., Etcoff, N., Ariely, D., Chabris, C. F., O’Connor, E., & Breiter, H. C. (2001). Beautiful faces have variable reward value: fMRI and behavioral evidence. Neuron, 32, 537-551.
Breiter, H. C., Aharon, I., Kahneman, D., Dale, A., & Shizgal, P. (2001). Functional imaging of neural responses to expectancy and experience of monetary gains and losses. Neuron, 30(2), 619-639.
Eysenck, H. J., & Eysenck, S. B. (1991). Manual of the Eysenck personality scales. Sydney: Hodder & Stoughton.
Fabian, A. (1990). Card sharps, dream books, & bucket shops: gambling in 19th-century America. Ithaca: Cornell University Press.
Kambouropoulos, N., & Staiger, P. K. (2001). The influence of sensitivity to reward on reactivity to alcohol-related cues. Addiction, 96, 1175-1185.
Kane, T. A., Loxton, N. J., Staiger, P. K., & Dawe, S. (2004). Does the tendency to act impulsively underlie binge eating and alcohol use problems? An empirical investigation. Personality and Individual Differences, 36, 83-94.
Powell, J. H., Al-Adawi, S., Morgan, J., & Greenwood, R. J. (1996). Motivational deficits after brain injury: Effects of bromocriptine in 11 patients. Journal of Neurology, Neurosurgery & Psychiatry, 60, 416-421.
Lyla Caldera December 10, 2011
Lyla Caldera
I loved your blog article.Really thank you! Really Great.