


Research suggests that increased heart rate is a psychophysiologic response to gambling activities like blackjack (Anderson & Brown, 1984), poker machine play (Coulombe et al., 1992; Dickerson et al., 1992; Leary & Dickerson, 1985), and horse racing (Coventry & Norman, 1997). However, no research has described gambling’s effect on stress hormone secretion, as well as this effect’s relationship with increased heart rate and pathological gambling severity (Meyer et al., 2000).
A study conducted by Meyer et al. (2000) examined heart rate and salivary cortisol secretion in a sample of male casino blackjack players (n=10) before, during, and after play. Participants were recruited within a real casino environment, each reporting that they play games of chance at least once per week. Study participants took part in experimental and control sessions. The experimental session required participants to be fitted with heart rate monitors and to provide a baseline saliva sample prior to blackjack play with their own money. Heart rate monitors began recording subsequent to situating players at a blackjack table. Second, third, and fourth saliva samples were collected thirty minutes, sixty minutes, and upon termination of play respectively. In addition, at the end of play, research participants were required to complete a questionnaire consisting of Likert-type assessments designed to measure the extent of their gambling addiction1. The control session was identical to the experimental session except that in the former session participants played a game of cards with no money at stake.
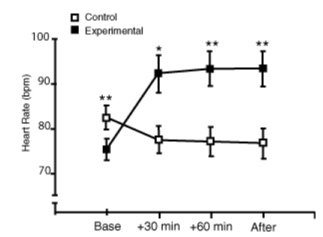
Meyer et al. (2000) found that blackjack gambling produced a significant increase in heart rate response throughout the experimental session. Indeed, as Figure A shows, heart rate lowered across the control session; heart rate increased from baseline to thirty minutes during the experimental session by an average of eighteen beats per minute (Meyer et al., 2000). In general, heart rate remained higher throughout the experimental session compared with the control session (Meyer et al., 2000).

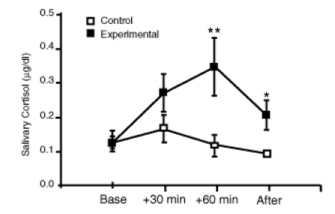
Salivary cortisol also was elevated during the experimental session (Meyer et al., 2000). The peak cortisol increase came after sixty minutes of gambling. Furthermore, while the levels dropped following the completion of the experimental session, these remained significantly higher than the levels at the end of the control session as Figure B indicates (Meyer et al., 2000).
In addition, Meyer et al. (2000) discovered that pathological gambling severity was negatively correlated with heart rate in the control condition (baseline, r = -.661, p = .038; +30 min, r = -.815, p =. 004; +60 min, r = -.830, p = .003; baseline r = -.859, p = .001). However, pathological gambling severity was unrelated to cortisol levels during the control session and to both cortisol and heart rate levels during the experimental session (p>.05). Moreover, Meyer et al. (2000) found inconsistent positive relationships between heart rate and salivary cortisol levels during blackjack play. Indeed, heart rate responses were linked with increased salivary cortisol levels at +30 minutes and post gambling, but not at +60 minutes (p<.05).
Meyer et al. (2000) make an important contribution to an otherwise sparse area of gambling research. However, their results might be biased by methodological weakness. For example, Meyer et al. (2000) measure heart rate and salivary cortisol levels in both the experimental and control conditions at a point in time referred to as the "end of play." However, the duration of time between the sixty-minute measurement and the "end of play" measurement goes unspecified. Indeed, some research participants might have played blackjack for longer than others after the sixty-minute measurement; this extension of play could have affected heart rate and salivary cortisol levels at the "end of play." Moreover, the control session is described as "a game of cards without any monetary stakes" (Meyer et al., p. 949, 2000). However, the researchers fail to specify whether this control "game" is blackjack or another type of card game. If the control session game was not comparable to blackjack, then conclusions about differences between the heart rate and salivary cortisol levels throughout the experimental and control sessions might be compromised.
In addition, other than blackjack, Meyer et al. (2000) did not consider other types of gambling during their research. By not considering other games (e.g., lottery, craps, or roulette), it becomes difficult to determine with scientific certainty whether the rise and fall of heart rate and salivary cortisol levels observed in both the experimental and control sessions are common to gambling or limited solely to blackjack.
Finally, the researchers conclude that pathological gambling severity is unrelated to cortisol and heart rate levels during the blackjack gambling session. The implications of this finding are very important. If this result is supported by future research, then valuable evidence is beginning to emerge about the neuroadaptation that intemperate gamblers experience. However, Meyer et al. (2000) base their conclusions about the relationships among heart rate, salivary cortisol, and pathological gambling severity on one research participant whose score was just above the study cut-off for a "severe gambling addiction."
Despite these limitations, Meyer et al. (2000) have opened the door to discoveries about important connections that might exist between some neurophysiological reactions and gambling behavior. While the research suggests that gambling has the potential to produce acute and stress-like endocrine responses (Meyer et al., 2000), it also indicates that the biological consequences of problem and pathological gambling are as vital to consider as the social, emotional, and economic consequences as scientists move toward an improved understanding of these behavior patterns.
1. A score of 16-25 on the questionnaire indicated an emerging gambling addiction; 26-45 a medium gambling addiction; 45-60 a severe gambling addiction.
References
Anderson, G., & Brown, R. I. (1984). Real and laboratory gambling, sensation seeking and arousal. British Journal of Psychology, 75, 401-410.
Coulombe, A., Ladouceur, R., Desharnais, R., & Jobin, J. (1992). Erroneous perceptions and arousal among regular and occasional video poker players. Journal of Gambling Studies, 8, 235-244.
Coventry, K. R., & Norman, A. C. (1997). Arousal, sensation seeking and frequency of gambling in off-course horse racing bettors. British Journal of Psychology, 88, 671-681.
Dickerson, M., Hinchy, J., England, S. L., Fabre, J., & Cunningham, R. (1992). On the determinants of persistent gambling behavior. I. High-frequency poker machine players. British Journal of Psychology, 83, 237-248.
Leary, K., & Dickerson, M. (1985). Levels of arousal in high- and low-frequency gamblers. Behaviour Research and Therapy, 23, 635-640.
Meyer, G., Hauffa, B. P., Schedlowski, M., Pawlak, C., Stadler, M. A., & Exton, M. S. (2000). Casino gambling increases heart rate and salivary cortisol in regular gamblers. Society of Biological Psychiatry, 48, 948-953.
The WAGER is a public education project of the Division on Addictions at Harvard Medical
School. It is funded, in part, by the National Center for Responsible Gaming, the
Massachusetts Department of Public Health, the Addiction Technology Transfer Center of
New England, the Substance Abuse and Mental Health Services Administration, and the
Center for Substance Abuse Treatment.