


Comings’ (1998) research on the genetic commonalities of pathological gambling and several other disorders suggested the former might be considered part of a spectrum disorder that defies the current, discrete diagnostic categories used in mental health (see WAGER 3:30). If the notion of a spectrum disorder is accepted, as Comings proposed, then DSM-IV’s classification of pathological gambling as an impulse disorder may require reconsideration. Of course, readers should not relegate their DSM-IVs to the recycling bin just yet. In addition to the fact that a radical revision is unlikely anytime in the near future, recent research by Steel and Blaszczynski (1998)2 lends a degree of credence to the placement of pathological gambling with kleptomania, intermittent explosive disorder, and other DSM-IV impulse disorders.
Using a sample of 82 gamblers seeking treatment at a clinic in Australia, Steel and Blaszczynski set out to investigate the relationships between measures of impulsivity, categories of personality disorder, and measures of pathological gambling as measured by the SOGS. By DSM-IV diagnostic criteria, all 82 gamblers were determined to be at the pathological level. To measure impulsivity, the authors used the Eysenck scale, which is composed of four subscales: impulsivity, risk-taking, non-planning, and liveliness. When mean subscale scores were computed (n=82) and compared to those of a normative sample (n=235), t-tests revealed statistically significant differences between the groups only for the subscales of non-planning (t=3.34, df=315, p<0.01) and impulsivity (t=4.28, df=315, p<0.001). The suspected correlation between impulsivity and pathological gambling has some support in the data.
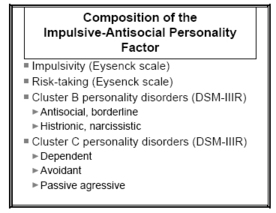
In the second phase of the study, the authors investigated the prevalence of established personality disorders in Cluster B personality disorders (DSM-IIIR) their sample. Subsequently, the authors proposed three personality types, each composed of a combination of impulsivity characteristics and clusters of personality disorders. Each of the three types was then entered into a regression analysis to determine their relative power for predicting SOGS scores. Only one of the three factor groups, the ‘impulsive-antisocial’ factor, was significantly correlated with the SOGS (r=0.33, F=9.43, df=1,71, p=<0.01; 2) The make-up of this group is presented in the table. Is the “impulsive-antisocial” personality type correlated with pathological gambling? Even if we were to unconditionally accept the findings discussed above, this in no way is tantamount to finding that “all pathological gamblers are impulsive and antisocial.” Finding a factor to be significantly correlated to a phenomenon is not the same as that factor being necessary for that phenomenon. And, as the authors point out, a correlation of 0.33 translates into an r2 of 0.10. That is, in the final analysis only 10% of the variance among SOGS scores can be explained by the impulsive-antisocial factor. In addition, as the authors recognize, their sample was composed exclusively of gamblers in treatment. There is no way to know whether the relationship found would hold true for the general population of compulsive gamblers. Lastly, although the cultures of Australia and the United States are relatively similar, the possibility exists that cross-cultural differences in the nature of gambling may complicate an American replication of these results.

Sources:
- Comings, D.E. (1998). The molecular genetics of pathological gambling. CNS Spectrums, 3(6), 20-37.
- Steel, Z., and Blaszczynski, A. (1998). Impulsivity, personality disorders and pathological gambling severity. Addiction, 93(6), 895-905.
This public education project is funded, in part, by The Andrews Foundation and the National Center for Responsible Gaming.
This fax may be copied without permission. Please cite The WAGER as the source.
For more information contact the Massachusetts Council on Compulsive Gambling