


The exact cause of gambling disorders is unknown. However, some research (e.g., Bergh, Eklund, Sodersten, & Nordin, 1997) has shown that altered dopamine function might be involved. Similarly, Parkinson’s disease is characterized by dopamine reduction that might incite certain cognitive and behavioral changes in those afflicted (Foti & Cummings, 1997). Molina et al. (2000) examine the association among pathological gambling, Parkinson’s disease, and Levodopa[1] therapy in a Spanish research sample.
Twelve research participants, eleven men and one woman, met criteria for pathological gambling and Parkinson’s disease according to DSM-IV and the Unified Parkinson’s Disease Rating Scale (UPDRS; Hoehn & Yahr, 1967), respectively. Investigators questioned the participants about their gambling behavior (e.g., age of gambling onset and preferred gambling activity) in addition to information about their gambling patterns before and after the onset of Parkinson’s disease.
The results revealed that research participants began gambling at approximately forty-seven years of age (Molina et al., 2000). Consistent with other Spanish gambling studies (e.g., Becona, 1997), the Parkinson’s patients’ preferred gambling activity was slot machines. They also played casino, bingo, and lotto games (Molina et al., 2000).
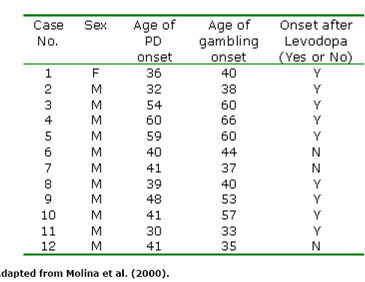
Data indicate that ten of twelve research participants reported that their gambling began sometime after the onset of the Parkinson’s disease (Molina et al., 2000). More specifically, data show that gambling behavior might be related to Levodopa therapy for Parkinson’s patients. Indeed, nine of twelve Parkinson’s patients began gambling after they began Levodopa therapy. Two patients who gambled before their Parkinson’s diagnosis and one who began Levodopa therapy preceding gambling onset reported a dramatic increase in gambling behavior once therapy began (Molina et al., 2000). Table 1 summarizes the possible relationship among pathological gambling, Parkinson’s disease, and Levodopa therapy.
Table 1. Clinical features of research participants diagnosed with pathological gambling and Parkinson’s disease (PD)*

Molina et al. (2000) posit some interesting results, most notably the relationship among Levodopa therapy and gambling behavior. However, this research is exploratory. The study sample is small and the findings might not generalize to other populations in Spain and abroad. Only one female is included in the research sample. Therefore, it is not possible to determine the extent to which this individual represents other female Parkinson’s patients.
Moreover, Molina et al. (2000) have not shown a statistical relationship between pathological gambling, Parkinson’s disease, and Levodopa therapy. Indeed, the researchers only report that an unspecified amount of gambling proceeded Parkinson’s onset, and that this gambling increased-again, in an unspecified amount-for most of the research participants when Levodopa therapy was introduced. While we know that the participants met criteria for pathological gambling according to DSM-IV at the time of the study, we do not know whether Levodopa therapy was partly or fully responsible for stimulating the behavior upon which this diagnosis rests, or whether additional biological, psychological, and/or social factors were involved. Despite these concerns, this research holds the promise to open other avenues for new theory, research, and treatment for gambling disorders.
[1] According to The American Heritage Dictionary of the English Language, Fourth Edition (2001), Levodopa is an amino acid that is the metabolic precursor of dopamine, converted in the brain to dopamine, and used in synthetic form to treat Parkinson’s disease.
References
Becona, E. (1997). Pathological gambling in Spanish children and adolescents: an emerging problem. Psychological Reports, 81, 275-287.
Bergh, C., Eklund, T., Sodersten, P., & Nordin, C. (1997). Altered dopamine function in pathological gambling. Psychological Medicine, 27, 473-475.
Foti, D. J., & Cummings, J. L. (1997). Neurobehavioral aspects of movements disorders. In R. L. Watts & W. C. Koller (Eds.), Movement Disorders, Neurologic Principles and Practice. (pp. 15-30). New York: McGraw Hill.
Hoehn, M. M., & Yahr, M. D. (1967). Parkinsonism: onset, progression and mortality. Neurology, 17, 427-442.
Molina, J. A., Sainz-Artiga, M. J., Fraile, A., Jimenez-Jimenex, F. J., Villanueva, C., Orti-Pareja, M., & Bermejo-P, F. (2000). Pathological gambling in Parkinson’s Disease: a behavioral manifestation of pharmacologic treatment. Movement Disorders, 15(5), 869-872.
The WAGER is a public education project of the Division on Addictions at Harvard Medical
School. It is funded, in part, by the National Center for Responsible Gaming, the
Massachusetts Department of Public Health, the Addiction Technology Transfer Center of
New England, the Substance Abuse and Mental Health Services Administration, and the
Center for Substance Abuse Treatment.