


High drop out rates can plague even the most well-designed addiction treatment programs. Recent research by Milton, Crino, Hunt, & Prosser (2002) addressed this issue by examining the efficacy of a compliance-improvement intervention (CII) as a supplement to Cognitive-Behavioral Therapy (CBT). This WAGER will examine the evidence that pertains to treatment completion.
At a local university gambling treatment center, the researchers recruited 47 individuals seeking treatment for pathological gambling. The inclusion criteria required participants to meet criteria for pathological gambling; researchers excluded seven potential participants for various reasons including: not being pathological gamblers, upcoming legal sentencing, and current use of antipsychotic medication. The remaining 29 male and 11 female participants were randomly assigned to receive CBT alone or CBT+CII. Each condition required a total of 8 structured therapy sessions. This consisted of 1 assessment session followed by 4 weekly sessions. These sessions were then followed by 3 bi-monthly sessions and a final session four weeks later. CBT consisted of psycho-education, cognitive restructuring, developing problem-solving skills, and relapse prevention. CII employed eight interventions intended to enhance and maintain gamblers’ motivation to change their gambling behavior and to complete treatment: (1) praise for making therapy appointments, (2) positive prognosis at the end of treatment, (3) emphasis on attending all treatment sessions, (4) appointment confirmation letters, (5) relaying assessment results, (6) requesting the completion of inter-session decision-balance sheets, (7) problem solving for change inhibiting behaviors, and (8) reinforcement of self-efficacy.
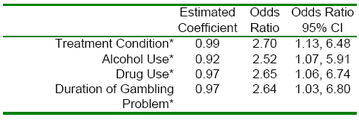
Sixty five percent of the CBT+CII group completed treatment and 35% of the CBT alone group completed treatment. Using logistic regression, the authors examined how well the treatment condition (i.e. CBT v. CBT+CII), pre-treatment alcohol use, pre-treatment drug use, and duration of gambling problem predicted treatment completion (Table 1). Individuals who drank, used alcohol, or had a gambling problem for a longer period were each about two and a half times less likely to complete treatment.
Table 1: Logistic Regression on Treatment Completion

* p<0.05.
This work is both important and interesting because it addresses a common concern of treatment providers, one that gambling researchers have not frequently focused upon: treatment dropout. This work tries to advance the benefits of CBT by offering a much needed tool for patient retention. However, this work does have some limitations. For example, the CII intervention is extensive and ranges from counseling content to mailed reminders. This makes it difficult to determine which aspects of CII are the most influential. The multiple components of CII might be experienced as additional treatment. Further, these multiple components might not be readily applied in treatment settings that do not have sufficient resources for such an initiative. Finally, programs that attempt to reduce patient dropout imply that dropping out is a problem. Although treatment completion is often associated with better outcomes, dropping out of treatment is not always an indicator of poor outcome. Individuals may leave treatment programs early because they have gleaned the necessary information for health. Nevertheless, Milton et al. provide a very important treatment study that highlights an all too common obstacle to healing.
Comments on this article can be addressed to Debi LaPlante.
References
Milton, S., Crino, R., Hunt, C., & Prosser, E. (2002). The effect of compliance-improving interventions on the cognitive-behavioral treatment of pathological gambling. Journal of Gambling Studies, 18(2), 207-229.