


The American Psychiatric Association diagnostic guidelines conceptualize pathological gambling (PG) as either present (five or more signs or symptoms) or absent (four or fewer signs or symptoms). This diagnostic scheme for PG weights all signs and symptoms equally. Many researchers and clinicians have suggested that a more continuous conceptualization, in which the diagnostic guidelines consider the severity of specific signs and symptoms, would be more appropriate for the disorder than this dichotomous unweighted approach. In this edition of the WAGER, we review a study by Strong & Kahler (2007) which investigated the psychometric properties of the 10 DSM-IV criteria, and evaluated the gambling severity continuum.
Strong and Kahler analyzed data from the National Epidemiologic Survey on Alcohol and Related Conditions (NESARC), a national general population survey of 43,093 adults that includes a DSM-IV-based measure of pathological gambling. The researchers applied a Rasch Model – an analysis that assesses the severity of symptoms and their probability of being endorsed by individuals at different places along a severity continuum of PG – to the 2,180 respondents who endorsed one or more lifetime PG criteria.
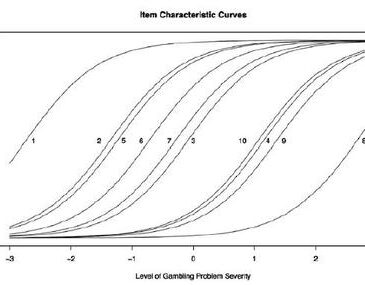
Figure 1. Probability of endorsing specific PG signs and symptoms at different levels of gambling problem severity (reproduced from Strong & Kahler, 2007).

Note. Level of Gambling Problem Severity is determined by the Rasch Model but corresponds roughly to number of symptoms endorsed. Each curve refers to a symptom: 1 = preoccupation w/ gambling; 2 = tolerance; 5 = escape; 6 = chasing; 7 = lying; 3 = loss of control; 10 = relying on others to cover debt; 4 = withdrawal; 9 = jeopardizing relationships; 8 = illegal acts.
Twelve percent of all gamblers endorsed being ‘preoccupied with gambling,’ and this problem fell in the mild range of the severity continuum; less than 0.1% of all gamblers endorsed committing “illegal acts to finance gambling,” and this problem fell at the most severe end of the continuum. Figure 1 shows the distribution of the 10 PG criteria along the dimension of gambling severity (i.e., # of symptoms endorsed). The symptoms are not equally distributed across the continuum; the figure also shows that, in some cases, a relatively larger increase in gambling severity is required before further gambling symptoms are observed. These gaps provide guidance about the relationship between specific symptoms and possible thresholds for different levels of gambling problem severity. Preoccupation (curve 1) appears to be a diagnostic gateway for other problems. Tolerance, escape, chasing, lying, and loss of control occur at similar severity levels, but a large increase in severity is required before reliance on others, withdrawal symptoms, jeopardizing relationships, or illegal acts occur.
This study’s main analyses utilized lifetime criteria for PG, which is a limitation. Lifetime measurements can be problematic because of memory recall problems and reinterpretation of past events, as well as other biases. An analysis of past year symptoms could possibly reveal a different structure to the data. Despite this limitation, this study suggests that, contrary the current unweighted dichotomous classification scheme for pathological gambling, gambling problems fall along a severity continuum and different signs and symptoms occur at different thresholds of severity.
What do you think? Comments should be addressed to Line Gebauer and Sarah Nelson.
References
Strong, D. R., & Kahler, C. W. (2007). Evaluating the continuum of gambling problems using the DSM-IV. Addiction, 102(713-721).
Mentalman May 14, 2008
This is an encouraging direction that I hope will find it’s way into the DSM as I think that it lends greater validity to the process of diagnosis.