



Pathological gambling is increasingly recognized by professional and lay communities as a mental health disorder that requires professional intervention. In addition to major therapeutic treatment strategies, including cognitive behavioral therapy, psychoanalysis, and psychopharmacology, a growing number of treatment opportunities recently have been developed. For example, in June 2000, a national think tank on state-funded gambling treatment programs identified 13 states with state-funded gambling treatment programs. Similarly, the National Council on Problem Gambling, whose mission includes increasing treatment opportunities for gamblers and their families, reports 34 state-affiliated chapters across the United States. Consequently, empirical investigations of the efficacy of traditional and newly established therapeutic techniques and treatment programs are important. But, what constitutes treatment efficacy? Blaszczynski, McConaghy & Frankova (1991) suggested that non-abstinent but controlled gambling is an acceptable outcome of treatment. The WAGER summarizes their study of the relationship between different gambling treatment outcomes and mental health.
Blaszczynski et al. (1991) followed 55 male and 8 female DSM-III diagnosed pathological gamblers from a pool of 120 pathological gamblers who had previously completed a 1-week gambling behavioral treatment program at a psychiatric unit. At follow-up, study participants identified themselves as abstinent, controlled, or uncontrolled gamblers.1 Eighteen participants identified themselves as abstinent, 25 as controlled, and 20 as uncontrolled. The study obtained information from the collateral informants of 14 abstainers and 14 controlled gamblers. The collateral informants contradicted only one self-reported controlled gambler. This gambler was reclassified as uncontrolled. The average number of months between treatment and follow-up was similar for all groups (Table 1). Follow-up participants completed a battery of questions pertaining to mental health and social functioning.2 Some of these questions also had been administered prior to treatment.
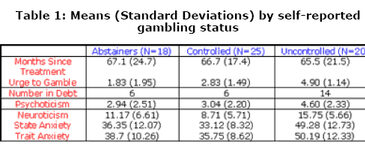
The gamblers who self-categorized themselves as abstainers, controlled gamblers, or uncontrolled gamblers at follow-up did not significantly differ from each other on most mental health measures taken prior to treatment.3 At follow-up, however, there were significant differences on the mental health measures (Table 1). No significant differences between abstainers and controlled gamblers were reported. However, the authors used the results of a three-group one-way analysis of variance (ANOVA) to suggest that compared to abstainers and controlled gamblers, uncontrolled gamblers reported significantly higher levels of psychoticism (p<0.05), neuroticism (p<0.01), state anxiety (p<0.01), and trait anxiety (p<0.01). Uncontrolled gamblers also reported a greater number of people in debt than abstainers and controlled gamblers.4 Finally, from a three-group one-way ANOVA, the authors suggested that uncontrolled gamblers reported a significantly higher urge to gamble than controlled gamblers and controlled gamblers reported a significantly higher urge to gamble than abstainers (p<0.01). The investigators did not report pair-wise comparisons testing the between group differences identified by the ANOVAs.
Table 1: Means (Standard Deviations) by self-reported gambling status

Former pathological gamblers who abstained from gambling at follow-up were in better mental health than those who continued uncontrolled gambling behavior. Interestingly, former pathological gamblers who maintained controlled levels of gambling at follow-up were in similar mental health as abstainers. From these results, it is possible to conclude that controlled gambling might be as acceptable an outcome of gambling treatment as abstinence.
The finding that abstaining and controlled gamblers maintained healthy mental health up to five years post treatment is promising. However, these results should be interpreted with caution for a number of reasons. First, this study relies on a relatively small sample size (i.e., only about half of the original cohort was evaluated at follow-up) and a particularly small number of women (i.e., only eight women were evaluated at follow-up). These matters question the potential stability and generalizability of the effects. Second, the researchers did not report analyses of pre-to-post treatment changes. These analyses would have added precision to the comparisons, as well as a description of how these subjects changed over time. Third, although many of the results were reported as if they were group-to-group comparisons (e.g. uncontrolled versus abstainers and controlled gamblers), the only analyses reported were omnibus ANOVAs that examined differences across all three groups. Post-hoc pair-wise comparisons or contrasts directly testing the presence of the observed overall effects were not reported. Fourth, although the authors reported post-treatment gambling behavior for abstainers alone and directly compared the behaviors of controlled and uncontrolled gamblers, a direct comparison of the post-treatment gambling behaviors of abstainers and controlled gamblers was not reported.
Perhaps the best method for comparing the success of abstainers and controlled gamblers would be to examine a broader range of outcomes such as the number of problem-level gambling relapses, time between problem-level gambling relapses, or the duration of extended gambling episodes. This evidence might reveal ongoing problems that would permit investigators to draw more precise conclusions about the efficacy of gambling treatment among controlled gamblers. Because controlled gamblers reported a significantly higher urge to gamble, this might make them more susceptible to lapses in normal gambling behavior.
Despite these concerns and suggestions, the results of Blaszczynski et al. (1991) are interesting; this research makes an important contribution to the scientific literature. Contrary to popular opinion, this research suggests that some individuals, who at one time had serious problems gambling, might be able to resume controlled levels of gambling after treatment and maintain mental health levels comparable with abstainers. With respect to mental health and other social functioning measures, it seems that treatment was not a "failure" for controlled gamblers. Should controlled gambling be universally viewed as an acceptable treatment outcome? That remains to be seen. More research is needed to determine whether there are other unmeasured consequences that distinguish these groups.
Notes
1 Abstinence was defined as no gambling in the month prior to follow-up and for the majority of the post-treatment period. Controlled gambling was defined as gambling without a “subjective sense of impaired control and adverse financial consequences.”
2 Mental health measures included the Eysenck Personality Questionnaire, the Sensation Seeking Scale, the State-Trait Anxiety Inventory, and the Beck Depression Inventory. These materials are cited in Blaszczynski et al. (1991). Authors also asked participants about gambling, health, marital status, and financial status.
3 Relative to controlled gamblers, significantly lower scores on the Sensation Seeking Scale were reported for uncontrolled gamblers.
4A c2 conducted for the WAGER revealed that the difference among the groups was significant (c2(2)=10.36, p<0.01).
References
Blaszczynski, A., McConaghy, N., & Frankova, A. (1991). Control versus abstinence in the treatment of pathological gambling: a two to nine year follow-up. British Journal of Addiction, 86, 299-306.
The WAGER is a public education project of the Division on Addictions at Harvard Medical
School. It is funded, in part, by the National Center for Responsible Gaming, the
Massachusetts Department of Public Health, the Addiction Technology Transfer Center of
New England, the Substance Abuse and Mental Health Services Administration, and the
Center for Substance Abuse Treatment.