The WAGER, Vol. 6 (45) – Look, But Don’t Touch: An Investigation Into Cue-Exposure, Response-Prevention Treatment
Ask seven addiction specialists to describe the best treatment for gambling addiction, and you might hear seven different answers. The diversity of thought regarding best practices for treatment highlights the importance of research focused on treatment outcomes. This week’s WAGER discusses a study that investigates the efficacy of cue-exposure and response-prevention as a treatment for problem gambling. Cue-Exposure, Response-Prevention assumes that reducing the strength of the association between triggers (i.e. seeing and hearing the slot machine) and urges to perform a behavior (i.e. gamble) will reduce the likelihood of that behavior being performed. The WAGER reviews the Symes and Nicki (1997) treatment program and its effect on gambling urges.
Symes and Nicki (1997) reported two case studies of a female and a male, St. Thomas University (Canada) undergraduates in their early twenties. Both young people scored as probable pathological gamblers on the South Oaks Gambling Screen (Lesieur & Blume, 1987).
Prior to treatment, the subjects participated in a baseline period to determine gambling patterns and tailor treatment strategy to each participant. The male participant’s baseline period was 26 days and he had only one 69-day treatment period. The female participant participated in an 11-day baseline period and two 69-day treatment periods. The participants also completed a Self-Efficacy Questionnaire (SEQ)1, which assessed the likelihood that they could avoid gambling in situations that might trigger them to gamble. Information from the baseline and the questionnaires was integrated into the treatment program.
Treatment began with two mock gambling sessions guided by researchers. Participants repeatedly (at least five times) used slot machines. However, when they did so their inserted coins were returned and no actual gambling took place. As part of their treatment, the participants were urged to notice the stimuli of the casino (i.e. the sound of the money in the machine, or the sight of other people winning) and record their reactions and the strength of their urges to gamble in gambling diaries. After the two initial sessions, the participants self-administered treatment whenever they felt an urge to gamble, or if they felt no urge, they were to administer treatment at least twice a week.
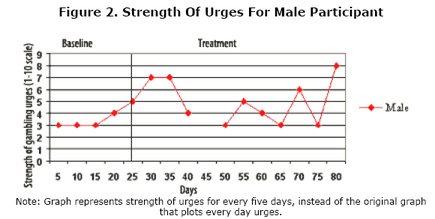
The strength of the female participant’s urges to gamble decreased substantially after her first treatment period. She evidenced only one spike in the strength of her urges before reporting no gambling urges during the last month of her treatment (Figure 1). However, for the male participant, the strength of gambling urges did not change appreciably (Figure 2).

Note: Graph represents strength of urges for every five days, instead of the original graph that plots every day urges.
Figure 2. Strength Of Urges For Male Participant
Note: Graph represents strength of urges for every five days, instead of the original graph that plots every day urges.
The female participant’s pattern of urges suggests that the association between gambling stimuli and gambling urges weakens as gambling-related behaviors are prevented from occurring. The male participant apparently did not respond to treatment. The researchers suggested that the male participant’s treatment might not have been effective because he had only one treatment period and a significant gap in that treatment period2.
Alternatively, it is possible that the treatment is ineffective and the success of the female participant occurred independent of this treatment effect. When first interviewed by the researchers, the female participant expressed a desire to stop gambling for financial reasons; the male participant, however, did not express any desire to stop or any concern over his gambling behavior. The reduction in her gambling urges might have been due primarily to her willingness to change, which happened to coincide with receiving treatment.
The results of this study suggest that the cue-exposure, response-prevention treatment approach needs much more investigation. This study examined only two subjects and the outcomes were inconsistent. A randomized empirical study with a much larger sample size is necessary before this treatment program can be utilized with any confidence.
In sum, the limitations of this study preclude drawing any meaningful conclusions regarding the efficacy of this treatment approach. However, since this approach has been used successfully with substance abusers to stop and prevent relapse, if further research shows that triggers can be “deprogrammed” in gamblers, cue-exposure and response prevention methods could be used to help gamblers change their behavior as well. In addition, this treatment strategy holds theoretical potential to guide the development of “safer” games by eliminating the elements that might reinforce maladaptive behavior (i.e. no bells, whistles, or lights). The work of Symes and Nicki represents an interesting contribution to the growing body of research on possible treatments for problem gamblers.
Notes
1 The Self-Efficacy Questionnaire was created by the researchers and based on a scale used to measure self-efficacy in smokers developed by Nicki, Remington, and MacDonald (1984).
2 The male participant went on March vacation from school in the middle of his treatment and did not follow the treatment program during his time off.
References
Lesieur, H.R. and Blume, S.B. (1987). The South Oaks Gambling Screen (SOGS): A new instrument for the identification of pathological gamblers. American Journal of Psychiatry, 44, 1184-1188.
Symes, Brent A. and Nicki, Richard M. (1997). A preliminary consideration of cue-exposure, response prevention treatment for pathological gambling behaviour: two case studies. Journal of Gambling Studies, 13(2), 145-157.
The WAGER is a public education project of the Division on Addictions at Harvard Medical
School. It is funded, in part, by the National Center for Responsible Gaming, the
Massachusetts Department of Public Health, the Addiction Technology Transfer Center of
New England, the Substance Abuse and Mental Health Services Administration, and the
Center for Substance Abuse Treatment.