The WAGER, Vol 4(31) – The National Gambling Impact Stusy Comission: Part I
On August 3, 1996, President Clinton signed Public Law 104-169, which authorized the creation of the National Gambling Impact Study Commission. This body was charged with conducting "a comprehensive legal and factual study of the social and economic impacts of gambling in the United States." The Commission, composed of nine members and chaired by Kay James, submitted its final report on June 18th of this year. Despite popular perception, the report is not a document dedicated exclusively to the study of pathological gambling. Its scope is much wider, and includes an assessment of the state of the gaming industry, a discussion of Native American tribal gaming, and other topics. However, perhaps the most
publicized findings of the report were those of a comprehensive study of problem and pathological gambling conducted by the National Opinion Research Center (NORC) at the University of Chicago. NORC, which since 1972 has conducted the seminal General Social Survey (GSS), interviewed nearly 2,500 adults by telephone, and an additional 530 subjects who were patrons at gambling establishments. A summary of the prevalence estimates they reported is presented in the table below. Data stratified by demographic group is also presented at the end of this WAGER.
NORC used DSM-IV criteria to guide the development of a new survey instrument. Respondents who had lost more than $100 in a single day and reported one or more DSM-IV criteria were classified as pathological, problem, or at-risk. While the former two categories are common in the gambling research literature, the at-risk classification is not. At-risk subjects were those who reported one or two criteria. The notion of "at-risk" is complex, and poses numerous problems for epidemiologists. Should the at-risk
group include anyone who has ever gambled? Should it include all those who live near a gambling venue? What about all persons who might ever travel to a gambling venue? Or what about all people? This issue is particularly salient when estimating prevalence. There is the classic example of the concept of "at-risk." Consider a cholera outbreak in a small country and the epidemiologist who must decide who is at-risk of contracting the illness. As the number of at-risk individuals increases, prevalence necessarily decreases. If 1,000 individuals are ill and all 100,000 citizens of the country are considered to be at risk, then the prevalence of cholera is 1%. If the at-risk group is expanded to inlcude the10,000,000 residents of neighboring countries, then the prevalence becomes 0.01%. If the entire world population is considered to be at risk, then the prevalence becomes infinitesimal. The complexity of this issue highlights the need for a standard nomenclature.
Overall, NORC estimated that 0.1% or 0.6% of the general adult population were pathological gamblers during the past 12 months, depending on whether patrons are included in the analysis. Both of these estimates are below those reported by studies conducted by Harvard Medical School (1997) and the National Research Council (1999). In addition, these prevalence estimates are considerably lower than estimates of past-year alcohol dependence/abuse (9.7%) and past-year drug dependence/abuse (3.6%).2
A primary purpose of the Commission was to inform public policy. Its findings may have ramifications for future regulation, research funding, and treatment. The exact nature of these ramifications remains to be seen. 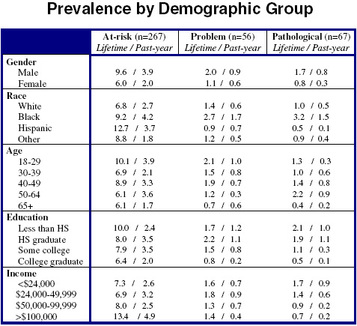
Sources: 1 National Gambling Impact Study Commission. (1999). National gambling impact study commission final report. Washington, DC: Author. 2 Kessler, R.C., McGonagle, K.A., Zhao, S., Nelson, C.B., Hughes, M., Eshleman, S., Wittchen, H., & Kendler, K.S. (1994). Lifetime and 12-month prevalence of DSM-III-R psychiatric disorders in the United States. Archives of General Psychiatry, 51, 8-19.
The WAGER is funded, in part, by the National Center for Responsible Gaming, the Massachusetts Department of Public Health, the Andrews Foundation, the Addiction Technology Transfer Center of New England, the Substance Abuse and Mental Health Administration Services, and the Center for Substance Abuse Treatment.